Abstract of the Milroy lectures on kala-azar, its differentiation and its epidemiology. Lecture I, The origin and course of the epidemic / by Leonard Rogers.
- Leonard Rogers
- Date:
- 1907
Licence: Public Domain Mark
Credit: Abstract of the Milroy lectures on kala-azar, its differentiation and its epidemiology. Lecture I, The origin and course of the epidemic / by Leonard Rogers. Source: Wellcome Collection.
9/16 page 488
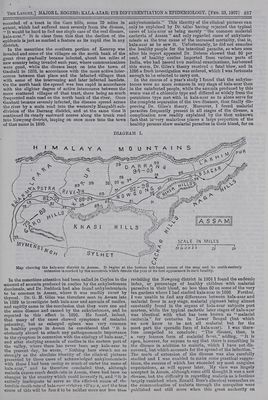
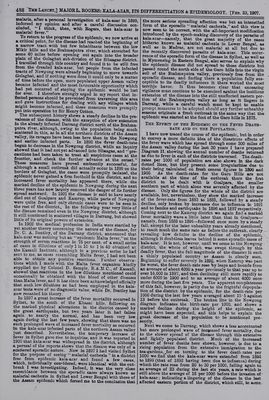
![* malaria, after a personal investigation of kala-azar in 1899, indorsed my opinion and after a careful discussion con- cluded, ‘‘I think, then, with Rogers, that kala-azar is malarial fever.” To return to the progress of the epidemic, we now arrive at a critical point, for the disease had reached the beginning of @ narrow tract with but few inhabitants between the low Mikir hills and the Brahmaputra river, which stretched for some 40 miles before opening out again into the broader plain of the Golaghat sub-division of the Sibsagas district, I travelled through this country and found it to be still free from the dreaded kala-azar, but people from the infected tracts of Nowgong were already beginning to move towards Golaghat, and if nothing were done it could only be a matter of time before the open, more populated upper Assam valley became infected and the most favourable opportunity which bad yet occurred of staying the epidemic would be lost for ever. I therefore strongly urged in my report that in- fected persons should be prevented from traversing this area and gave instructions for dealing with any villages which might become infected, and these measures were promptly put into operation by Sir Henry Cotton. valence of the disease, with the exception of slow extension _ in the already infected Darrang district north of the Brahma- putra river, although, owing to the population being much ‘scattered in this, as in all the northern districts of the Assam valley, its ravages have been less here than in the Nowgong and earlier infected parts. In 1898 the fever death-rate began to decrease in the Nowgong district, while an inquiry showed that it had not yet advanced into Sibsagas, and “ pre- cautions had been taken to treat all suspicious cases at the These measures have proved eminently successful, for although a small outbreak did actually occur in 1899 on the borders of Golaghat, the cases were promptly isolated, the epidemic never gained a firm foothold in this district, and no increased fever mortality has appeared there, while -the marked decline of the epidemic in Nowgong during the next three years has now largely removed the danger of its further spread eastward. In 1901] the disease is said to have nearly died out of Goalpara and Kamrup, while parts of Nowgong were quite free, and only chronic cases were to be seen in the rest of the district.. In the following year very little of the disease remained even in the Nowgong district, although it still continued in scattered villages in Darrang, but showed little of its original powers of extension, In 1902 the medical profession in India were startled by yet another theory concerning the nature of the disease, for Dr. C. A. Bentley, of the Darrang district, announced that kala-azar was nothing but an ‘‘epidemic Malta fever,’ on the strength of serum reactions in 75 per cent. of a small series of cases in dilutions of only lin 10 to 1 in 40 obtained at the Kasauli Institute, although in a previcus series he had sent to mé, as cases resembling Malta fever, I had not been able to obtain any positive reactions. Further observa- supplied me by Colonel D. Semple, R.A.M.C., of Kasanli, showed that reactions in the low dilutions mentioned could occasionally be obtained with the blood of other diseases than Malta fever, and it has since been acknowledged officially that such low dilutions as had been employed in the kala- azar tests were of no diagnostic value, while Dr. Bentley has now recanted his theory. In 1897 a great increase of the fever mortality occurred in Sylhet, to the south of the Khasai hills, following on the marked physical alterations in the district caused by the great earthquake, but two years later it had fallen again to nearly the normal, and has been very low again during the last few years, showing that there was no such prolonged wave of increased fever mortality as occurred in the kala-azar infected parts of the northern Assam valley just described. Nevertheless, the temporary increase of fever in Sylhet gave rise to inquiries, and it was reported in 1900 that kala-azar was widespread in the district, although a perusal of the reports shows that the disease was only of a scattered sporadic nature. Now in 1897 I had visited Sylhet for the purpose of seeing ‘‘ malarial cachexia ” in a district free from epidemic kala-azar and found a few cases, which, individually considered, were identical with the out- break I was investigating. Indeed, it was the very close resemblance between the sporadic cases always known as malarial cachexia in Sylhet and Lower Bengal with those of the Assam epidemic which forced me to the conclusion that the more serious spreading affection was but an intensified form of the sporadic ‘* malarial cachexia,” and this view is now seen to be correct, with the all-important modification introduced by the epoch-making discovery of the parasite of kala-azar—namely, that the great majority of the cases hitherto known as malarial cachexia in Lower Bengal, as well as in Madras, are not malarial at all but due to the recently discovered parasite of kala-azar. This occur- rence of the sporadic form of the disease in Sylhet, as well as in Mymensing in Eastern Bengal, also serves to explain why the epidemic disease did not spread to those districts but passed round the north side of the Garo hills into the virgin soi] of the Brahmapntra valley, previously free from the sporadic disease, and finding there a population fully sus- ceptible to its deadly influences it there worked the most terrible havoc. It thus becomes clear that unceasing vigilance must continue to be exercised against the insidious extension of the disease into the still unaffected eastern por- tion of the Brahmaputra valley as long as it lingers in Darrang, while a careful watch must be kept to enable prompt measures to be adopted should any further unhealthy seasons originate a fresh outbreak in the same way that the epidemic was started at the foot of the Garo hills in 1875. THE EFFECT OF THE EPIDEMIC ON THE FEVER DEATH- RATE AND ON THE POPULATION. 1 have now traced the course of the epidemic, but in order to convey a more definite idea of the disastrous effects of the fever wave which has spread through some 300 miles of the Assam valley during the last 30 years I have prepared Diagram IT. showing the annual number of deaths returned as due to fever in each of the districts traversed. The death- rates per 1000 of population are also shown in the dark dotted lines, but they present some irregularities due to their being calculated on fresh census figures in 1890 and 1900. As the death-rates for the Garo Hills are not available at the time of the outbreak there the first . district to be dealt with is Goalpara, the smaller southern part of which alone was severely affected by the disease. Only the figures for the whole of. the district are available, but, nevertheless, they show the marked increase . of the fever-rate from 1883 to 1888, followed by a steady decline, only broken by increases due to influenza in 189] and to famine and earthquake in 1896 and 1897 respectively. Coming next to the Kamrup district we again finda marked fever. mortality wave a little later than that in Goalpara— namely, from 1888 to 1894—followed once more by a steady fall, except for the’ later unhealthy years already mentioned, to reach much the same rate as before the outbreak, clearly — revealing how definite is the decline of the epidemic, although it doubtless leaves behind it some sporadic cases of kala-azar. It is not, however, until we come to the Nowgong’- district, the whole of which. was swept through by this. deadly fever, that the full magnitude of the disaster in such. a thinly populated country as Assam is clearly seen. Beginning to suffer severely in 1892, when Kamrup was past its worst, the fever death-rate rose by leaps and bounds from an average of about 4000 a year previously to that year up to. under 6000 in 1900 and to an average of about 4000 once: more during the last five years. The apparent completeness. of this fall, however, is partiy due to the frightfal depopula- tion of the district by the epidemic, for the death-rate per 1000 during the last few years averaged about 15°5 against 13 before the outbreak. The broken line in the Nowgong diagram indicates the birth-rate per 1000, and shows a. marked decline during the height of the epidemic, as. might have been expected, and this helps to explain the great decrease of the population to be mentioned pre-- sently. - Next we come to Darrang, which shows a less accentuated but more prolonged wave of incyeased fever mortality, due to the slower spread of the disease through this extensive and lightly populated district. Much of the increased: number of fever deaths here shown, however, is due to a rising population from the extensive immigration to the tea-gardens, for on turning to the fever death-rates per 1000 we find that the kala-azar wave extended from 1804 to 1899 (that of 1892 having been due to influenza) during which the rate rose from 20 to 30 per 1000, falling again to an average of 23 during the last six years, a rate which is still above the average of 18 per 1000 before the invasion of kala-azar ; indicating a lingering of the disease in the last affected eastern portion of the district, which still, to sume..](https://iiif.wellcomecollection.org/image/b33450523_0009.jp2/full/800%2C/0/default.jpg)