Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz.
- Haab O. (Otto), 1850-1931.
- Date:
- 1899
Licence: Public Domain Mark
Credit: Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
206/312 (page 158)
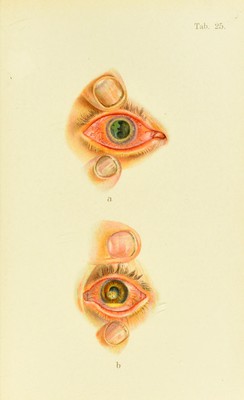
![Plate 25. a. Herpes corneae febrilis, three weeks after the beginning of the dis- ease, stained with fluorescin, showing a green ulcer, of irregular, sinuous shape, in the temporal half of the cornea. (The green color is a little too light in the figure.) A slight degree of vessel-formation may be seen at the temporal margin of the cornea. The conjunctiva is stained yellow by the flnoresciu and, in addition, shows marked ciliary congestion. The pupil is dilated with atrojiin. b. Hypopyon-keratitis.—Just below the center of the cornea is a puru- lent infiltration which developed in the course of a few days. The limit of the infiltration remains stationary. The hypopyon in the anterior chamber is 2 mm. high. No history of traumatism. There are moderate dacryosteuosis and chronic conjunctival catarrh. Satisfactory cure after several applications of pure carbolic acid. Visual acuity §. of gastric fever suffices to bring it out. The malady is ]iarticularly common after influenza. In spite of tlie long duration of the process, tlie iris rarely becomes involved, unle.ss a secondary infection takes place. The diagnosis is readily made from the symptoms dc- .scribed, and e.specially from the color obtained vith fluo- rescin. Sometimes a herpetic ulcer fails to .sliow the typical sinuous contour (re.^^embling a geograj)hica\ map), in which case we base our diaguo.sis on the slow proee.ss of repair. At first the di.seased s[)ots may easily be mistaken for scratches, exeept for the absence of a history of trau- matism. It is often diffieult to determine the febrile nature of the disea.se, because the patients usually present themselves long after they have forgotten any feverish .sym])toms they may have had. Occasionally a herjK'tic macula from a former attack is detected and helps to clear up the diagnosis. Prognosis.—We should emjfliasize the ])robability of a long duration, and, if the Ivsion is centrally situated, the unavoidable ])crmanent impairment of vi.sion. On ‘'the other hand, if the ulcer is properly treated there is little danger of its spreading. Relapses are not infre- quent, and little or nothing can be done to prevent their occurrence.](https://iiif.wellcomecollection.org/image/b21691587_0206.jp2/full/800%2C/0/default.jpg)