Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz.
- Haab O. (Otto), 1850-1931.
- Date:
- 1899
Licence: Public Domain Mark
Credit: Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
286/312 (page 212)
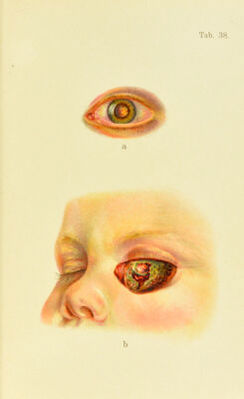
![Plate 38. a and h. Glioma of the Retina.—The infant was quite well up to the sixth month of its existence, at which time she began to squint with the left eye. When she was one year old her mother noticed a yellowish reflex in the pupil, which appeared more and more distinct as the pupil dilated. A few weeks ago (the child is now twenty months old) the right eye began to show signs of failing vision. The left eye was somewhat inflamed, hard (T f 1), and larger than the right. The left iris brown, the right blue. Left pupil dilated and rigid, transmitting a bright reflex (sec Fig. a) corresponding to several nodules which appeared to occupy the greater portion of the vitreous. The surface of the tumor streaked with red, partly blood-vessels and partly, no doubt, hemor- rhages. In the right eye, in which tension was normal, the pupil was dilated and there was a coinjilete, fuunel-shaped retinal separation ; tlie eye appeared to be nearly blind. Enucleation of botli eyeballs was proposed and refused; but the child was brought back one year later to have the operations performed. At this time there was marked protrusion of the left eye; the cornea was increased to twice its normal size and was opaque; two days after admission it ruptured and large masses of the tumor protruded through the opening (Fig. b). Four days after admis- sion, enucleation on the right side and extirpation of the contents of the orbit on the left were performed. On account of severe hemorrhage, however, it was impossible to sterilize the orbit thoroughly in the region of the optic foramen ; on the next day fever set in, and on the day following, scarlet fever. Death two weeks after the operation, from purulent meningitis. Periostitis of the orbit i.s quite freqnenlly met with. Its usual seat is tlie margin, where it produees thiekeniiig and tenderness on pressure, d'he thickened masses ot bone are not movable. Often there is edematous swelling of the lids. An inflammation situated in the posterior j)ortion of the orbit is less easily recognized and often very difficult to distinguish from orbital cellulitis. It manifests itself by jirotrusion, with more or less pain, and lessened mobility of the eyeball (Plate 39). Sometimes the nature of the process is not recognized until a deep-seated perios- titis leads to snpjmration and the abscess ruptures an- teriorly, when the roughness of the bone is felt with the probe. The su])purative process may spread to the cra- nium and cause meningitis or cerebral abscess. This complication is particularly apt to follow periostitis of the](https://iiif.wellcomecollection.org/image/b21691587_0286.jp2/full/800%2C/0/default.jpg)