Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz.
- Haab O. (Otto), 1850-1931.
- Date:
- 1899
Licence: Public Domain Mark
Credit: Atlas of the external diseases of the eye : including a brief treatise on the pathology and treatment / by O. Haab ; Authorized translation from the German, edited by G.E. de Schweinitz. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
298/312 (page 220)
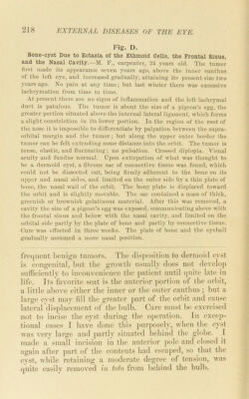
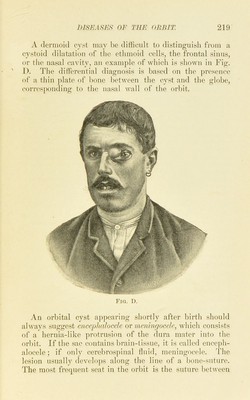
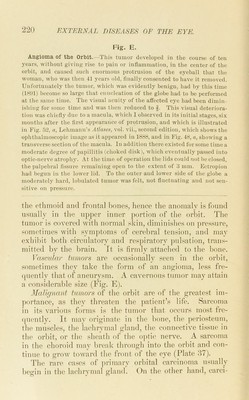
![Fig. E. Angioma of the Orbit.--This tumor developed in the course of ten j'ears, without giving rise to pain or inflammation, in the center of tlie orbit, and caused such enormous protrusion of tlie eyeball that the woman, who was then 41 years old, finally consented to have it removed. Unfortunately the tumor, which was evidently benign, had by this time (1891) become so large that enucleation of the globe had to be performed at the same time. The visual acuity of the afl’ected eye had been dimin- ishing for some time and was then reduced to f. This visual deteriora- tion was chiefly due to a macula, which I observed in its initial stages, six months after the first appearance of protrusion, and which is illustrated in Fig. .52, a, Lehmann’s Atlases, vol. vii., second edition, which shows the ophthalmoscopic image as it appeared in 1888, and in Fig. 48, n, showing a transverse section of the macula. In addition there existed for some time a moderate degree of papillitis (choked di.sk), which eventually pa-ssed into optic-nerve atrophy. At the time of operation the lids could not be closed, the palpebral fissure remaining open to the extent of 3 mm. Ectropion had begun in the lower lid. To the outer and lower side of the globe a moderately hard, lobulated tumor was felt, not fiuctiiating and not sen- sitive on pressure. the ethmoid and frontal bones, hence the anomaly is found usually in the upper inner jiortion of the orbit. The tumor is covered with normal skin, diminishes on jiressnre, sometimes with .symptoms of cerebral tension, and may exhibit both circulatory and respiratory jinlsation, trans- mitted by the brain, ft is firmly attached to the bone. \Ai,sciUar tumors are occasionally seen in the orbit, sometimes they take the form of an an_i>;ioma, le.ss fre- (piently that of anenrysm. A cavernous tumor may attain a (ionsiderable size (Fi^. E). MaUejnant tumors of the orbit are of the greate.st im- portance, as they threaten the ])atient’s life. Sarcoma in its various forms is the tumor that occurs most fre- (piently. It may originate in the bone, the periosteum, the muscles, the lachrymal gland, tlie connective tis.sne in the orbit, or the sheath of the ojitie nerve. A sarcoma in the choroid may break through into the orbit and con- tinue to grow toward the front of the eye (Plate 87). The rare cases of iirimary orbital carcinoma nsnally begin in the lachrymal gland. On the other hand, carci-](https://iiif.wellcomecollection.org/image/b21691587_0298.jp2/full/800%2C/0/default.jpg)