Volume 1
A text-book of human physiology : including histology and microscopical anatomy : with special reference to the requirements of practical medicine / by L. Landois ; translated from the seventh German edition, with additions, by William Stirling.
- Date:
- 1891
Licence: Public Domain Mark
Credit: A text-book of human physiology : including histology and microscopical anatomy : with special reference to the requirements of practical medicine / by L. Landois ; translated from the seventh German edition, with additions, by William Stirling. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
120/602 page 80
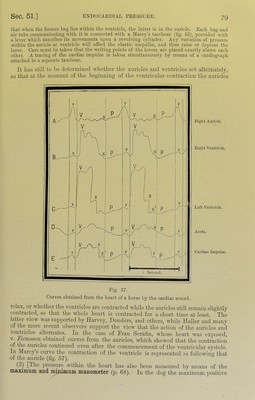
![pressure in tlie left ventricle is during systole greater tliau that in tlie aorta, and may reach 140 mm. Hg—tliat in the riglit ventricle 60 mm., and tlie right auricle about 20 mm. Hg. The minimum manometer, hov'ever, during the diastole of the ventricles records a negative pressure of - 52 to - 20 mm. Hg in the left and - 16 mm. in the right ventricle, and - 7 mm. in the right auricle. Even after the chest is opened, the negative pressure in the left ventricle may fall as low as - 25 mm. Hg.] [(3) Method of Rolleston and Roy.—These observers used a special apparatus which was con- nected with the interior of the heart, and they find that there is no distinct rise of pressure in the dog within the ventricles corresponding to the auricular systole such as was obtained by Marey in the horse. During the ventricular diastole in certain cases the pressure falls below the atmosiiheric pressure and may be equal to - 20 mm. mercury or more in the left ventricle (§ 48). It is probably caused by the elastic expansion of the ventricle continuing after the blood in the auricle at the moment of the cessation of the ventricular systole has entered the ventricle—i.e., the quantity of blood in the auricle is not sufficient in all cases to disteiid the left ventricle to the point at which its suction action ceases. Magiiii, operating on dogs with a trocar which perforated the cavities of the heart, found none of the secondary elevations obtained by Marey with his sound. There is considerable difficulty in interpreting the curves obtained (fig. 50, B).] A. Fiek regards the alternating contraction as a means whereby the pressure in the large venous trunks is kept nearly constant. At the moment of ventricular systole the auricles relax, and the venous blood flows freely into the latter, while if the auricles remained contracted, the blood in the veins would be kept back. Further, at the moment of ventricular diastole the auricles contract, so that there is not an abnormal diminution of the pressure in the veins. Thus the pressure in the auricle is more equable, while the current in the terminal parts of the veins is kept more constant. 52. PATHOLOGICAL CARDIAC IMPULSES.—Change in the Position of the Apex-Beat.— The position of the cardiac impulse is changed—(1) by the accumulation of fluids (serum, jjus, blood) or gas in one pleural cavity. A copious efl’usion into the left pleural cavity compresses the lung, and may displace the heart towards the right side, while effusion on the right side may push the heart more to the left. As the right heart must make a greater effort to propel the blood through the compressed lung, the cardiac impulse is usually increased. Advanced emphysema of the lung, causing the diaphragm to be pressed downwards, displaces the heart downwards and inwards, while pushing and pulling up of the diaphragm (by contraction of the lung, or through pressure from below) causes the apex-beat to be displaced upwards, and also slightly to the left. Thickening of the muscular walls with dilatation of the cavities of the left ventricle makes that ventricle longer and broader, while the increased cardiac impulse may be felt in the axillary line in the sixth, seventh, or even eighth intercostal .space to the left of the mammary line. Hypertrophy, with dilatation of the right side, increases the breadth of the heart, so that the cardiac impulse is felt more to the right, even to the right of the sternum. In the rare cases where the heart is transposed, the apex- beat is felt on the right side. When the cardiac impulse goes to the left of the left mammary line, or to the right of the parasternal line, the heart is iucreasetl in breadth, and there is hypertrophy of the heart. A greatly increased cardiac impulse may extend to several inter- costal spaces. The cardiac impulse is abnormally weakened in cases of atrophy and degeneration of the cardiac muscle, or by weakening of the innervation of the cardiac ganglia. It is also weakened when the heart is separated from the chest-wall owing to the collection of fluids or air in the pericardium, or by a greatly distended left lung ; and, indeed, when the left side of the chest is filled with fluid, the cardiac impulse may be extinguished. The same occurs when the left ventricle is very imperfectly filled during its contraction (in consequence of marked narrowing of the mitral orifice), or when it can only empty itself very slowly and gradually, as during marked narrowing of the aortic orifice. An increase of the cardiac impulse occurs during hypertrophy of the walls, as well as under the influence of various stimuli (psychical, inflammatory, febrile, toxic) which nflect the cardiac ganglia. Great hypertrophy of the left ventricle causes the heart to heave, so that a part of the left'chest-wall may be raised and also vibrate during systole. . , , • , A pulling in of the anterior wall of the chest during the cardiac .systole occurs in the third and fourth interspaces, not unfrequeutly under normal circumstances, sometimes during in- creased cardiac action, and in eccentric hypertrophy of the ventricles. As the heart’s apex is sli<^htly displaced, and the ventricle becomes slightly smaller during its systole, the empty space is filled by the yielding soft parts of the intercostal space. When the heart is united with the pericardium and the surrounding connective-tissue, which renders systolic locomotion of the heart impossible, retraction of the chest-wall during systole takes the place ot the](https://iiif.wellcomecollection.org/image/b21981516_0001_0120.jp2/full/800%2C/0/default.jpg)
 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image