[Report 1947] / Medical Officer of Health, Dorking U.D.C.
- Dorking (England). Urban District Council.
- Date:
- 1947
Licence: Attribution 4.0 International (CC BY 4.0)
Credit: [Report 1947] / Medical Officer of Health, Dorking U.D.C. Source: Wellcome Collection.
26/45 page 23
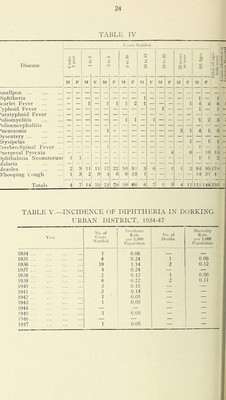
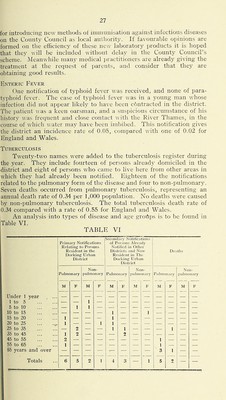
![6.—PREVALENCE OF, AND CONTROL OVER, INFECTIOUS DISEASE notifiabek infectious disease Table IV shows the nuinljer of cases of infectious diseases notilied during 1947, classified according to age and sex, together with tlie number of patients removed to isolation liospital, and the number of deaths, if any, from the various diseases. Smaplpox.—No case of small])ox was notified during the year. No primary vaccination or re-vaccination was performed by tire l^Iedi- cal Officer of Health under the Public Health (Smallpox Prevention) Regulations, 1917. Vaccination.—It may be noted that one of the results of the National Health Service Act will be the abolition of compulsory vac- cination, and of the appointment of public vaccinators. Instead, local health authorities, in this area the vSurrey County Council, are required to make a scheme for providing vaccination for all who seek it. The County Council proposes that the treatment should be given either by the applicant’s own doctor or 1>y its jiulilic health staff, at the nearest Iiealth centre. At the request of the County Council, the local super- vision of the scheme and the keeping of records have l)een made tlie duty of the Urban District Council’s Medical Officer of Healtli. ScARivET Fever.—Eight notifications were received during the year, compared with thirteen in 1946. The case-rate was 0.39 i)er 1,000 dvilian population, conq)ared with 1.37 for England and Wales. All af the patients were admitted to hospital for treatiqent. Diphtheria.—One case of diphtheria was notified, the case-rate ivas 0.05 per 1,000 civilian population, compared w ith 0.14 for England md Wales. The patient concerned was a boy aged eleven years, living n and going to a school at Westcott. He had ))een immunised five :ears previously. While there was no doul)t as to the nature of the lisease, the cour.se of the illness was undoul)tcdly modified to tlie latient’s advantage by the jiartial immunity wliich he no doubt retained rom the treatment. F'ollowing the occurrence of tliis case sjiecial fforts were quickly made in We.stcott to immunise or re-immunise as iiany children as possible who required treatment. Despite con- iderable investigation the source of the infection was not traced. No ther cases were reported. The downward tendency of diplitlieria incidence and mortality ates will be noticed on reference to Table V, in wliich arc tabulated :ie yearly figures since 1934. In my opinion this .satisfactory feature ; the result of several factors, of which I consider the more important 3 be the improved general care of children’s health, both in the ome and at school; the speedy and en'ccti\'c stei)s taken in co-o|)cration V medical practitioners, the school medical authority ami tlie local nblic health dc])artmcnt in detecting and isolating suspected sources f infection; and, imrticularly in the last few years, in the eoiitrolled roduction of immunisation by appropriate treatment.](https://iiif.wellcomecollection.org/image/b29164928_0027.jp2/full/800%2C/0/default.jpg)