Atlas and abstract of the diseases of the larynx / by L. Grünwald ; authorized translation from the German edited by Charles P. Grayson.
- Ludwig Grünwald
- Date:
- 1902
Licence: Public Domain Mark
Credit: Atlas and abstract of the diseases of the larynx / by L. Grünwald ; authorized translation from the German edited by Charles P. Grayson. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
76/284 page 70
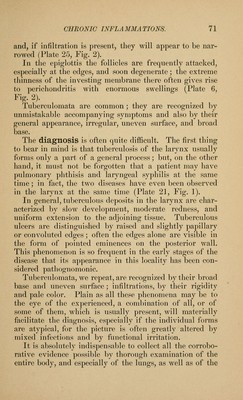
![generation is more likely to occur where function has be- come impaired, the infiltration extending far beyond the limits of the visible ulcer (Plate 20). In some cases the tubercle-formation proceeds for a long time within the deep layers, and occasionally gives rise to non-specific proliferations in the epithelial and mucous layers. These appear as swellings and are usu- ally found to consist also of diseased tissue. The pro- liferations may lead to the formation of actual tumors, their true nature being masked by the intact appearance of the surface and the presence of a pedicle (Plate 21, Fig. 2; Plate 21, Fig. 1; Plate 26, Fig. 2; Plate 28, If the perichondrium is more extensively invaded, there result edematous swellings, and later necroses, pre- fera])lv in the cricoid and arytenoid cartilages, correspond- ing to the most frequent localization in the mucous mem- brane of the posterior Avail. All these various anatomical features are very often blended in a strange ])icture of deformity and devastation. I/aryngOSCOpic Image.—In the initial stages we often see round or pointed eminences projecting from the interarvtenoidean region, beneath which ulceration may liave already begun. These projections are usually pale ; in fact, the entire larynx and even the fauces are usually anemic : there are, however, many exceptions to this rule. Sometimes the process first betrays itself by paresis or redness of one or both true vocal cords. These also may be the seat of slight hypertrophies and excres- cences. If the infiltration in the vocal cords breaks down, we see discolored yellow, and sometimes, from pro- trusion of the granulated background, reddish erosions with more or less swollen or uneven edges (Plate 12, Fig. 2; Plate 21, Fig. 2). The decubital action of the other vocal cord leads to com]>lete longitudinal fission of the affected one, so that it ajipears to be divided into an upper and a lower half (Plate 16, Fig. 2). The false vocal cords are usually somewhat thickened.](https://iiif.wellcomecollection.org/image/b21220463_0076.jp2/full/800%2C/0/default.jpg)





 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image