Auricular fibrillation and its relationship to clinical irregularity of the heart / by Thomas Lewis.
- Thomas Lewis
- Date:
- [1910?]
Licence: In copyright
Credit: Auricular fibrillation and its relationship to clinical irregularity of the heart / by Thomas Lewis. Source: Wellcome Collection.
25/80 (page 327)
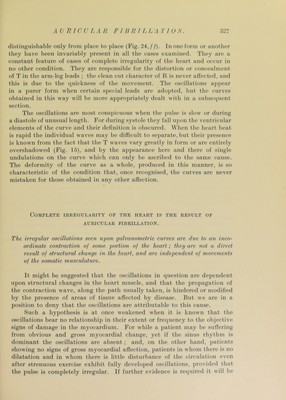
![distinguishable only from place to place (Fig. 24:, f f). In one form or another they have been invariably present in all the cases examined. They are a constant feature of cases of complete irregularity of the heart and occur in no other condition. They are responsible for the distortion or concealment of T in the arm-leg leads ; the clean cut character of R is never affected, and this is due to the quickness of the movement. The oscillations ap])ear in a purer form when certain special leads are adopted, but the curves obtained in this way will be more appropriately dealt with in a subsequent section. The oscillations are most conspicuous when the ])ulse is slow or during a diastole of unusual length. For during systole they fall upon the ventricular elements of the curve and their definition is obscured. When the heart beat is rapid the individual waves may be difficult to separate, but their presence is known from the fact that the T waves vary greatly in form or are entirely overshadowed (Fig. 15), and by the appearance here and there of single undulations on the curve which can only be ascribed to the same cause. The deformity of the curve as a whole, produced in this manner, is so characteristic of the condition that, once recognised, the curves are never mistaken for those obtained in any other affection. Complete irregularity of the heart is the result of AURICULAR FIBRILLATION. The irregular oscillations seen upon galvanometric curves are due to an inco- ordinate contraction of some portion of the heart; they are not a direct result of structural change in the heart, and are independent of mox'ements of the somatic muscidature. It might be suggested that the oscillations in question are dependent upon structural changes in the heart muscle, and that the propagation of the contraction wave, along the path usually taken, is hindered or modified by the presence of areas of tissue affected by disease. But we are in a position to deny that the oscillations are attributable to this cause. Such a hypothesis is at once weakened when it is known that the oscillations bear no relationship in their extent or frequency to the objective signs of damage in the myocardium. For while a patient may be suffering from obvious and gross myocardial change, yet if the sinus rhythm is dominant the oscillations are absent ; and, on the other hand, ])atients showing no signs of gross myocardial affection, patients in whom there is no dilatation and in whom there is little disturbance of the circulation even after strenuous exercise exhibit fully developed oscillations, provided that the pulse is completely irregular. If further evidence is required it will be](https://iiif.wellcomecollection.org/image/b29000610_0025.jp2/full/800%2C/0/default.jpg)