Auricular fibrillation and its relationship to clinical irregularity of the heart / by Thomas Lewis.
- Thomas Lewis
- Date:
- [1910?]
Licence: In copyright
Credit: Auricular fibrillation and its relationship to clinical irregularity of the heart / by Thomas Lewis. Source: Wellcome Collection.
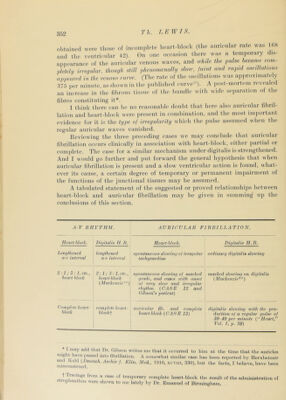
52/80 page 354
![this was tlie cliief lesion ; but here again itis ol)viousthat attention lias been eoncentrated upon a limited portion of the musculature. Amongst the cases belonging to this investigation one only has come to autojisy. It was a case of sti’eptococcic endocarditis, and a large area of ulceration was found on the seiital wall of the left auricle. I have since seen, through the kindness of Major-General F. Smith, a case of irregularity in a horse. The irregularity was complete, as shown by tracings, and a systolic ])ulsation was ajijiarent in the veins of the neck and reached the angle of the jaw while the animal was standing. Great breathlessness and dro])sy vere ])resent. The dis- turbance of the heart’s rhythm was of eight months’duration. An examina- tion of the heart showed considerable hy])ertro])hy of the ventrieles and auricles ; it was esjiecially marked in the latter. The endocardium of the left ventricle and auricle was oj)ac[ue and thickened ; there were large and scattered patches of sub-])ericardial fibrosis in the left auricle, but in no other part of the musculature. (The histology will be reported at a later date.) It is possible that fibrosis, by interfering evith the circulation in restricted areas of the musculature, sets up a state of irritability. The tendency for anaemia of the muscle to bring about new ini])idse formation is readily demonstrated experimentally. Ligation of a branch of a coronary artery is usually followed by the a])pearance of extrasystoles''’. Jlut it is difficult to suppose a constant state of anaemia in the affected tissues, and an anaemia of long duration. It must also be remembered that extensive fibrosis may occur without irregularity'b Some light seems to be thrown u])on the question by an examination of the relation of fibrillation to extrasystoles. There a])])ear to be two ty])es of case of the ]iaroxysmal affection. A type in which the interludes ai’e characterised by a perfect regularity of the heart {CAS h JO), and n type in which the regular rhythm of the slow period is interrupted by extrasystoles {(\\SES 2 and 11). In my own limited experience the extrasystoles which interru])t the slow periods, or those which intei’inipt the normal rhythm ])rioi’ to the onset of the fibiillation, have been auricular in origin {(WSKS 2 ami 11). rheir ])i‘esence in these ])atients and in certain oi those rep<n'ted by -Mackenzie arrests attention. Me cannot divorce the j^roblems of tlu' factors influencing the origin of single and multiple ectopic impulses, neithei- can wt‘ separate these (picstions fio;n that ot the origin of fibrillation. The production of a single new impulse, of a series of im])ulses from a single focus,or of multi})le im])idses liom scatteied foci, is a juatter of degree. Furthermore, we cannot excvdj^ate vhese single ectopic beats. 1 hey apj)ear to])artici))ate in producingtheultimate ciisis. In the eases obseiv^ed they have been very numerous. In the last number of this Journal a case was described in w Inch auricular extrasystoles wt ic as nunu ious as normal beats, and in this patient jiaroxysms of ectopic leats weic seen, which also arose in the auricle. On one oeeasion while a paroxysm was in ])rogress the auricle ])assed into fibrillation ; and after 1 s duration for about half a minute the auricular })aroxysm reappeared.](https://iiif.wellcomecollection.org/image/b29000610_0052.jp2/full/800%2C/0/default.jpg)



 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image