The dissector's manual of practical and surgical anatomy / By Erasmus Wilson.
- William James Erasmus Wilson
- Date:
- 1856
Licence: Public Domain Mark
Credit: The dissector's manual of practical and surgical anatomy / By Erasmus Wilson. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
44/594 page 50
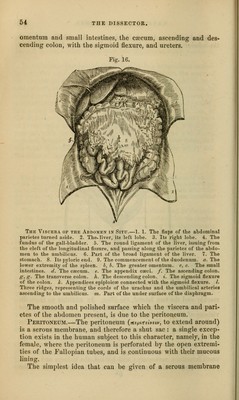
![Intep:ument, Superficial fascia, Intercolumnar fascia, Conjoined tendon, Transversalis fascia, Peritoneal sac. Direct inguinal hernia differs from oblique, firstly, in never at- taining the same bulk, in conse- quence of the resisting nature of the conjoined tendon of the inter- nal oblique and transversalis, and of the transversalis fascia; secondly, in its direction, having a tendency to protrude from the middle line, rather than towards it; thirdly, in making for itself a new passage through the abdominal parietes, instead of following a natural channel; and fourthly, in the re- lation of the neck of its sac to the epigastric artery, that vessel lying to the outer side of the opening of the sac of direct hernia, and to the inner side of that of oblique hernia. All the forms of inguinal hernia are designated scrotal, when they have descended into that cavity. Oblique inguinal hernia, in its course through the spermatic canal, lies above the spermatic cord. In rare cases the hernial protrusion may separate the components of the cord, so that some of them may lie in front of the tumor: hence one of many reasons for extreme care and caution in operating for strangu- lated hernia. Direct inguinal hernia often carries the spermatic cord before it, so that the vessels of which it is composed be- come spread over the front of the hernial sac, or slip to one side. In operating upon inguinal hernia, the importance of knowing the layers which cover it, and which are to be cut through be- fore reaching the bowel, is obvious; the oblique and direct her- nia differ from each other in this respect only in the composition of the fourth layer, the cremastcr occui>ying that place in oblique hernia, and the conjoined tendon in direct. If the oblique in- guinal hernia had reached no further than the spermatic canal, then the a])oneurosis of the external obli{|ne muscle would take the place of the intercolumnar fascia. This form of oblique in- guinal hernia is termed bubonocele. Encysted Herxia; the Her- nial Sac containing the Intes- tine BEING BEHIND THE TuNlCA Vaginalis.—1. The hernial sac. 2. The cavity of the tunica vagi- nalis. 3. The testicle. 4. The spermatic cord. The arrow shows that three laj'ers of serous mem- brane must be divided before the intestine can be reached.](https://iiif.wellcomecollection.org/image/b20998831_0044.jp2/full/800%2C/0/default.jpg)