The dissector's manual of practical and surgical anatomy / By Erasmus Wilson.
- Wilson, Erasmus, Sir, 1809-1884.
- Date:
- 1856
Licence: Public Domain Mark
Credit: The dissector's manual of practical and surgical anatomy / By Erasmus Wilson. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
74/594 (page 80)
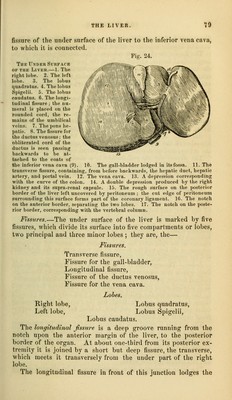
![fibrous cord of tlie umbilical vein, and is generally crossed by a band of hepatic substance called the pons hepatis. The Jissiwe for the ductus venosus is the shorter portion of the lonp:itudinal fissure, extending from the junctional termination of the transverse fissure to the posterior border of the liver, and containing a small fibrous cord, the remains of the ductus veno- sus. This fissure is, therefore, but a part of the longitudinal fissure. The transverse fissure is the short and deep fissure, about two inches in length, through which the hepatic ducts quit, and the hepatic artery and portal vein enter the liver. Hence this fissure was considered by the older anatomists as the gate (porta) of the liver; and the large vein entering the organ at this point, the portal vein. At their entrance into the transverse fissure the branches of the hepatic duct are the most anterior, next those of the artery, and most posteriorly the portal vein. The fissure for the gall-bladder is a shallow fossa extending forwards, parallel with the longitudinal fissure, from the riglit extremity of the transverse fissure to the free border of the liver, where it frequently forms a notch. The fissure for the vena cava is a deep and short fissure, occa- sionally a circular tunnel, which proceeds from a little behind the right extremity of the transverse fissure to the posterior border of the liver, and lodges the inferior vena cava. These five fissures taken collectively resemble an inverted v» the base corresponding with the free margin of the liver, and the apex with its posterior border. Viewing them in this war, the two anterior branches represent tlie longitudinal fissure on the left, and the fissure for the gall- bladder on the right side; the two posterior, the fissure for the ductus venosus on the left, and the fissure for the vena cava on the right side ; and the connecting bar, the transverse fissure. Zohes.—The nght lobe is four or six times larger than the left, from which it is separated on the concave surface, by the longi- tudinal fissure, and, on the convex, by the longitudinal ligament. It is marked upon its under surface by the transverse fissure, and by the fissures for the gall-bladder and vena cava; and presents three depressions, one, in front, for the curve of the ascending colon (imprcssio colica), and two, behind, for the right supra- renal cai)sule and kidney (inipressio renalis). The left lobe is small and flattened, convex upon its ujiper sur- face, and concave below, where it lies in contact with the ante- rior surface of the stomach. It is sometimes in contact by its extremity with the upper end of the spleen, and is in relation, by its ])osterior border, with the cardiac orifice of the stomach aiul left pnouniogastric nerve. The lobus (juadratns is a quadrilateral lobe situated on the](https://iiif.wellcomecollection.org/image/b20998831_0074.jp2/full/800%2C/0/default.jpg)