Licence: Public Domain Mark
Credit: Caries of the tarsus and ankle-joint. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
5/8 page 33
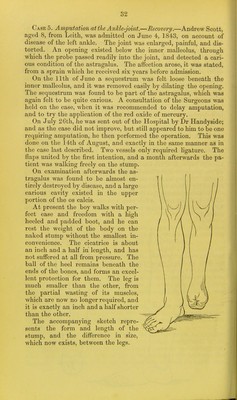
![S3 Remarks.—The two cases first related occurred at a period when, for caries of the tarsus and ankle-joint, amputation through the leg was regarded as the established practice here as elsewhere. In Cases 1 and 3, amputation was performed not immediately below the knee, as most surgeons recommend, but in accordance with the recommendation of Professor Fergusson of London, through, or rather below, the middle of the leg; as in my opinion, also, this part should be selected in preference to the former, when the sur- geon has his choice. The danger to life is thus less, the stump, if well formed, is equally comfortable, and afterwards the limb is more serviceable, owing to the patient having free use of the knee- joint. In Case 3, although previously the importance of amputation at the ankle-joint for caries occurring there, had been demonstrated by Professor Syme, and although the latter operation had been, as already stated, previously performed by myself, I preferred, for Tea- sons already given, amputating a few inches higher up. It was after- wards seen that, as far as the bones were concerned, the operation at the ankle-joint might have been performed, but previously the efficacy of it seemed to me so doubtful, as not to warrant the attempt. Moreover, the danger attending the operation which was performed, though greater than that incurred by the operation at the ankle- joint, is not, I believe, as already stated, nearly so great as that which attends amputation immediately below the knee, which ope- ration most surgeons would have regarded as the alternative in these circumstances; and I regretted the less being obliged to amputate through the middle of the leg, as after the latter opera- tion the limb, with the appropriate apparatus attached to it, is equally useful to the patient as after amputation at the ankle-joint, the motions of the knee being equally preserved in both. The operation of amputation through the leg is no doubt more dangerous to life than that at the ankle-joint,—as is shown by the fact, that out of upwards of twenty cases in which the operation has been performed in this city, all the patients except one have recovered. But it appears to me to be an important observation, which is well illustrated by the results of the operations in Cases ]' 2, and 3, that the disproportion in the fatality would be much de- creased^ were we to reckon only those cases of amputation through the leg in which the operation at the ankle-joint might have suf- ficed. And accordingly, most of the fatal cases in which the former operation had been performed, would be found to be those where the latter was quite inapplicable, such as for acute gangrene of the foot—for severe injuries at the ankle, attended with exten- sive contusion and laceration of the soft parts—and for necrosis, severe compound fractures, &c, occurring in the lower or middle thirds of the leg, which do not by any means generally require am- putation through the thigh or above the knee.](https://iiif.wellcomecollection.org/image/b21695714_0007.jp2/full/800%2C/0/default.jpg)