Volume 1
Operative gynecology / by Howard A. Kelly.
- Howard Atwood Kelly
- Date:
- 1901, ©1898
Licence: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Credit: Operative gynecology / by Howard A. Kelly. Source: Wellcome Collection.
Provider: This material has been provided by The University of Glasgow Library. The original may be consulted at The University of Glasgow Library.
552/622 (page 506)
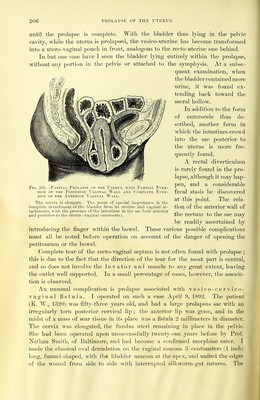
![until the prolapse is complete. With the bladder thus lying in the pelvic cavity, while the uterus is prolapsed, the vesico-uteriiie has become transformed into a utero-vaginal pouch in front, analogous to the recto-uterine one behind. In but one case have I seen the bladder lying entirely within the prolapse, without any portion in the pelvis or attached to the symphysis. At a subse- quent examination, when tlie bladder contained more urine, it was found ex- tending back toward the sacral hollow. In addition to the form of enterocele thus de- scribed, another form in which the intestines ci-owd into the sac posterior to the uterus is more fre- quently found. A rectal diverticulum is rarely found in the pro- lapse, although it niay hap- pen, and a considerable fecal stasis be discovered at this point. The rela- tion of the anterior wall of the rectmn to the sac may be readily ascertained by introducing the finger within the bowel. These various possible complications must all be noted before operation on account of the danger of opening the peritoneum or the bowel. Complete tear of the recto-vaginal septum is not often found with prolapse ; this is due to the fact that the direction of the tear for the most part is central, and so does not involve the levator ani muscle to any great extent, leaving the outlet well supported. In a small percentage of cases, however, the associa- tion is observed. An unusual complication is prolapse associated ^\■ith vesico-cervico- vaginal fistula. I operated on such a case April 9, 1892. The patient (K. W., 1320) was fifty-three years old, and had a large prolapsus sac with an irregularly torn posterior cervical lip ; the anterior lip was gone, and in the midst of a mass of scar tissue in its place was a fistula 2 millimeters in diameter. The cervix was elongated, the fundus uteri remaining in place in the pelvis. She had been operated upon unsuccessfully twenty-one years before by Prof. Nathan Smith, of Baltimore, and had become a confirmed morphine eater. I made the classical oval denudation on the vaginal mucosa 3 centimeters (1 inch) long, funnel-shaped, with tlie bhwlder mucosa at the apex, and united the edges of the wound from side to side with iiiterru])te(l sillvwoi-m-gut sutures. The Fig. 292.—Paktial Prolapse of the Uterus, with Partial Ever- sioN OF the Posterior Vaginal Wall and Complete Ever- siON OF THE Anterior Vaginal Wall. The cervix is elongate. The point of special importance is the complete detachment of the bladder from its uterine and vaginal at- tachments, with the presence of the intestines in the sac both anterior and posterior to the uterus (vaginal enterocele).](https://iiif.wellcomecollection.org/image/b21466099_0001_0570.jp2/full/800%2C/0/default.jpg)