Volume 1
Operative gynecology / by Howard A. Kelly.
- Howard Atwood Kelly
- Date:
- 1901, ©1898
Licence: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Credit: Operative gynecology / by Howard A. Kelly. Source: Wellcome Collection.
Provider: This material has been provided by The University of Glasgow Library. The original may be consulted at The University of Glasgow Library.
566/622 (page 520)
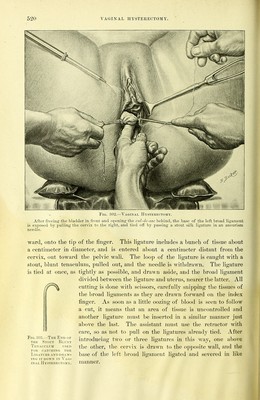
![Vaginal IJysterkcto.my. After freeinsr the bladder in front and opening' the cul-de-sac behind, the base of the left broad ligament is exposed by pulling the cervix to th« right, and tied off by passing a stout silk ligature in an aneurism needle. ward, onto the tip of the finger. This ligature inchides a Imnch of tissue about a centimeter in diameter, and is entered about a centimeter distant from the cervix, out toward the pelvic wall. The loop of the ligature is caught with a stout, blunt tenaculum, pulled out, and the needle is withdrawn. The ligature is tied at once, as tightly as possible, and drawn aside, and the broad ligament divided between the ligature and uterus, nearer the latter. All cutting is done with scissors, carefully snipping the tissues of the broad ligaments as they are drawn foi-ward on the index finger. As soon as a little oozing of blood is seen to follow a cut, it means that an area of tissue is uncontrolled and another ligature nnist be insei'tcd in a similar manner just above the last. The assistant must use the retractor with care, so as not to pull on the ligatures already tied. After introduciiig two or thi'ee ligatures in this way, one above the other, the cervix is drawn to the op])osite wall, and the base of the left broad liojament ligated and severed in like Fifi. 303.—The End or THE Stout Blunt Tenaculum used roil catching the Ligature and draw- ing IT DOWN IN Vag- inal JI YSTEUECTO.M V. manner.](https://iiif.wellcomecollection.org/image/b21466099_0001_0584.jp2/full/800%2C/0/default.jpg)