The science and art of surgery : being a treatise on surgical injuries, diseases, and operations / by John Erichsen ; edited by John H. Brinton.
- John Eric Erichsen
- Date:
- 1854
Licence: Public Domain Mark
Credit: The science and art of surgery : being a treatise on surgical injuries, diseases, and operations / by John Erichsen ; edited by John H. Brinton. Source: Wellcome Collection.
Provider: This material has been provided by the National Library of Medicine (U.S.), through the Medical Heritage Library. The original may be consulted at the National Library of Medicine (U.S.)
89/936
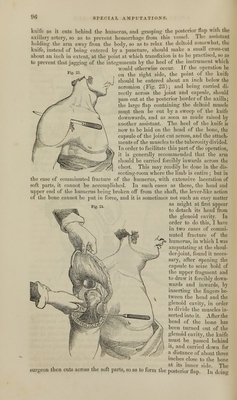
![this, the assistant to whom this duty is intrusted, must follow the knife with his hands, grasping firmly the whole thickness of the posterior flap, so as to compress the axillary artery, and thus prevent the occurrence of hemorrhage (Fig. 24). The surgeon should not cut the flap across until m the assistant tells him that he holds the vessel firmly, and then he must be cautious not to injure his assistant's fingers. The artery will he found to be cut long in the middle of the posterior flap, and a few smaller branches may be required to be tied at its inner angle and in the deltoid. The stump, after it is healed, will present the appearance in Fig. 25, taken from my last patient. In those cases in which this operation requires to be performed for diseases, especially for tumors of the humerus, it may very conveniently be done by making the anterior flap by cutting from without inwards, using of course for this purpose, a shorter knife than that which is required for transfixion. The joint is then opened, and the posterior flap formed in the usual way. [The oval operation of Baron Larrey has been most frequently performed, and has been attended with the best results. It consists in making a ver- tical incision of three inches in length, from the extremity of the acromion directly downwards in the axis of the humerus, splitting the deltoid muscle into two portions. From this vertical incision, about one inch below the acromion, two oblique incisions are carried, the anterior of which shall divide the tendon of insertion of the pectoralis major, and the posterior those of the latissimus dorsi and teres major. The soft parts are then strongly retracted by an assistant, so as to expose the articulation; the outer circumference of the capsule, with its tendons, is divided, the arm luxated outwards, and the division of the inner portion effected, an assistant compresses the axillary artery by grasping it between his finger and thumb, and the surgeon finishes the operation, by introducing his catling into the inferior ends of the oblique incisions, and incising, in a somewhat downward direction, the remaining soft parts and the skin. In this process, the axillary artery is last severed.—Ed.] Amputations of the foot. The phalanges of the toes seldom require amputation; when they do, they may be removed in the same way as the corresponding parts in the/ hand—by the formation of a flap on the plantar surface, either by cutting from above downwards, or by transfixion. In removing a bone at the metatarso-phalangeal articulation the oval method should always be practised, so that the sole of the foot may not be cut into. In doing this, it must be remembered that the articulation is situated at least three- fourths of an inch above the web of the toes, and the incision must therefore be commenced proportionately far backwards. The metatarsal bone of the great toe occasionally requires removal in whole or in part. If the disease is limited to the anterior part, the shaft of the bone should be cut across with a pair of bone-nippers, and its head left; for as this gives insertion to the peroneus longus, its removal will materially weaken the foot. The whole of the bone may be readily removed in the following way : the point of a strong broad bistoury should be entered on the dorsum of the foot in the interspace between the first and second metatarsal bones, as far back as pos- sible ; it should then be carried forwards upon the ball of the great toe to a point opposite to-the web between the toes, and thence made to sink into the sole of 7](https://iiif.wellcomecollection.org/image/b21118139_0089.jp2/full/800%2C/0/default.jpg)




 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image