A text-book of the practice of medicine.
- Anders, James M. (James Meschter), 1854-1936
- Date:
- 1913
Licence: Public Domain Mark
Credit: A text-book of the practice of medicine. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
56/1390 page 48
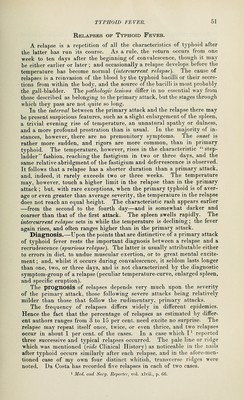
![Chantemesse' suggests an ophthalmic test, but the cutaneous reaction is a more simple test and gave positive results in every case in which it was employed (Deehan). C B. Burke^ has described a new reflex sign. Prendergast proposes a new typhoid fever test consisting in the injection with a fine hypodermic needle of a few drops of a suspension of dead typhoid bacilli of the strengtli of less than 5,000,000 per c.c. No reaction occurs in tyjdioid infection, but in the non-typhoid patient a well-marked area of redness around the injection develops within twenty- four hours. The cases that begin Avith the well-defined local inflammatory lesions previously referred to (tonsillo-typhoid, pneumo-typhoid, pleuro-typhoid, nepliro-ty])hoid) cannot be recognized at the outset. The same local inflammatory conditions may, independently of typhoid fever, be com- bined with a genuine typhoid state. In all instances of typlioid fever in which, at the time of onset, localization occurs, the degree of fever and prostration are apt to be out of pi-oportion to the local symptoms, and the former are apt to continue after the subsidence of the latter. A careful observation of the symptoms after the first week will usually detect undoubted symptoms of typhoid. The Widal test decides these cases. Blood-cultures if made early will also set the diagnosis at rest. The bacilli may be obtained from the stools and urine. Differential Diagnosis.—(1) Typhus fever (rarely met with) is to be dif- ferentiated by its appearance as an epidemic, by its sudden onset, by the deeper stupor, the besotted expression of tlie features, the injected con- junctivae, the contracted pupils, the appearance on the fourth day of macula; which are transformed into petechit« ; by the shorter course, the termination by crisis, and the absence of the Widal reaction. (2) Acute miliary tuberculosis is to be differentiated from typhoid fever by the greater frequency of the pulse and respirations, the cough, and in some instances by the expectoration; by the diff'use cyanosis and the presence (sometimes) of choroidal tubercles. Blood-exaniinations may show leukocytosis, but the large mononuclears are not increased as in typhoid fever. There is an absence of the temperature-curve, the pulse, the characteristic eruption, and the Widal reaction and abdominal symp- toms of typhoid. In doubtful cases lumbar puncture and blood-cultures should be undertaken, as tubercle or typhoid bacilli may be found. (.3) Malarial fever may assume the continued form of fever—e. g., the festivo-antumnal type, in which chills may be absent—and there are typhoids that affect both remittent and intermittent malarial fevers. Malaria can be differentiated from typhoid fever only by the detection of Laverans hematozoa in the blood. Should tjipho-malarial fever be suspected and the typhoid symptoms be unequivocal, the finding of the malarial organism would establish the diagnosis and diff'erentiate the hybrid from pui-e typhoid. (4) Relapsing fever is distinguished by its abrupt onset, with rigor, high fever, pain in the epigastrium ; by its brief duration, termination by crisis, and the occurrence of a relapse at the end of a week ; by the absence of the characteristic eruption and the sero-reaction of typhoid. The finding of the spirilla discriminates relapsing fever. (5) Meningitis.—In striking contrast with the specific typhoid symp- ^ Progressive Medicine, March, 1910, p. 1S6. ^New York Med. Jn>jr., Deo. 16, 1911.](https://iiif.wellcomecollection.org/image/b21229867_0056.jp2/full/800%2C/0/default.jpg)
 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image