Text-book of nervous diseases for physicians and students / by H. Oppenheim.
- Date:
- 1911
Licence: In copyright
Credit: Text-book of nervous diseases for physicians and students / by H. Oppenheim. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
45/1480 page 21
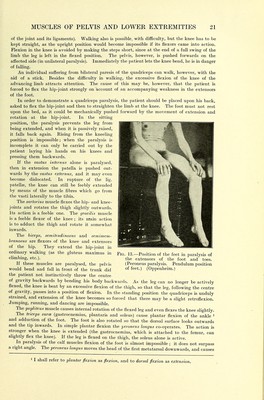
![of the joint and its ligaments). Walking also is possible, with difficulty, but the knee has to be kept straight, as the upright position would become impossible if its flexors came into action. Flexion in the knee is avoided by making the steps short, since at the end of a full swing of the limb the leg is left in the flexed position. The pelvis, however, is pushed forwards on the affected side (in unilateral paralysis). Immediately the patient lets the knee bend, he is in danger of falling. An individual suffering from bilateral paresis of the quadriceps can walk, however, with the aid of a stick. Besides the difficulty m walking, the excessive flexion of the knee of the advancing limb attracts attention. The cause of this may be, however, that the patient is forced to flex the hip-joint strongly on account of an accompanying weakness in the extensors of the foot. In order to demonstrate a quadriceps paralysis, the ]iatient should be placed upon his back, asked to flex the hip-joint and then to straighten the limb at the knee. The foot must not rest upon the bed, as it could be mechanically pushed forward by the movement of extension and rotation at the hip-joint. In the sitting position, the paralysis prevents the leg from being extended, and when it is passively raised, it falls back again. Rising from the kneeling position is impossible; when the paralysis is incomplete it can only be carried out by the patient laying his hands on his knees and pressing them backwards. If the vastus internus alone is paralysed, then in extension the patella is pushed out- wards by the vastus externus, and it may even become dislocated. In rupture of the lig. patellae, the knee can still be feebly extended by means of the muscle fibres which go from the vasti laterally to the tibia. The sartorius muscle flexes the hip- and knee- joints and rotates the thigh slightly outwards. Its action is a feeble one. The gracilis muscle is a feeble flexor of the knee ; its main action is to adduct the thigh and rotate it somewhat inwards. The biceps, semitendinosus and semimem- branosus are flexors of the knee and extensors of the hip. They extend the hip-joint in ordinary walking (as the gluteus maximus in climbing, etc.). If these muscles are paralysed, the pelvis would bend and fall in front of the trunk did the patient not instinctively throw the centre of gravity backwards by bending his body backwards. As the leg can no longer be actively flexed, the knee is bent by an excessive flexion of the thigh, so that the leg, following the centre of gravity, passes mto a position of flexion. In the standing position the quadriceps is unduly strained, and extension of the knee becomes so forced that there may be a slight retroflexion. Jumping, running, and dancing are impossible. The popliieus muscle causes internal rotation of the flexed leg and even flexes the knee slightly. The triceps surce (gastrocnemius, plantaris and soleus) cause plantar flexion of the ankle ^ and adduction of the foot. The foot is also rotated so that the dorsal surface looks outwards and the tip inwards. In simple plantar flexion the peroneus longus co-operates. The action is stronger when the knee is extended (the gastrocnemius, which is attached to the femur, can slightly flex the knee). If the leg is flexed on the thigh, the soleus alone is active. In paralysis of the calf muscles flexion of tlie foot is almost impossible ; it does not surpass a right angle. The peroneus longus moves the head of the first metatarsal downwards, and causes Fig. 13.—Position of the feet in paralysis of the extensors of the foot and toes. (Peroneus paralysis. Pendulum position of feet.) (Oppenheim.) 1 I shall refer to plantar flexion as flexion, and to dorsal flexion as extension.](https://iiif.wellcomecollection.org/image/b21981590_0045.jp2/full/800%2C/0/default.jpg)