Essentials of gynæcology : arranged in the form of questions and answers ; prepared especially for students of medicine / by Edwin B. Cragin.
- Cragin, Edwin B. (Edwin Bradford), 1859-1918
- Date:
- 1893
Licence: Public Domain Mark
Credit: Essentials of gynæcology : arranged in the form of questions and answers ; prepared especially for students of medicine / by Edwin B. Cragin. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
163/190 page 169
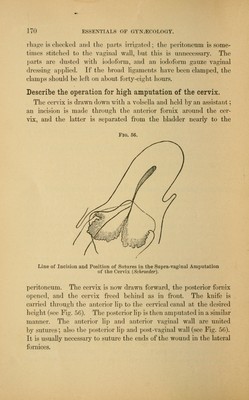
![rial walls, either hysterectomy or high amputation of the cervix may be performed. Authorities differ in their choice of the two opera- tions, the preference at the present time being most often given to hysterectomy. 2. Palliative.—When a radical operation is contraindicated, the following methods of treatment are of value :— If hemorrhage is a marked symptom, and sloughing masses are present at the seat of ulceration, thoroughly curette the surface and apply carbolic acid, iodized phenol, or a solution of chloride of zinc. Frequent insertions of iodoform gauze soaked in a 4 per cent, solu- tion of chloral will be found to act as an antiseptic and anaesthetic to the ulcerated surface. For the foul discharges, vaginal douches of a weak solution of creo- lin are valuable. The pain and distress in the later stages demand opium. Attention to the general health is of course indicated. Describe briefly the operation of vaginal hysterectomy. Different operators differ somewhat in the details of the operation. The main features of the operation are as follows: The vulva is shaved, and the vagina and vulva thoroughly disinfected. The uterus is drawn down and held by an assistant; a semicircular incision is made around the cervix in the anterior fornix, and the cervix is separated from the bladder up to the utero-vesica] pouch of the peritoneum. The cervix is drawn forward and the posterior fornix opened by a semicircular incision about the cervix, which is then freed up to the pouch of Douglas. The pouch of Douglas may now be opened, and a clean sponge, with a silver wire attached, introduced to keep back the intestines. The uterus is freed from the lower portion of the broad ligaments by clamping or ligaturing in section, and then cutting with scissors close to the uterus. The latter may now be retroverted through the opening in the pouch of Douglas, and freed from the upper portion of the broad ligaments by clamping or ligaturing, and cutting close to the uterus. It is well to draw the ovaries into the clamp or ligature, so that they will be removed with the uterus. The anterior reflection of peritoneum may now be divided, or, as practiced by many opera- tors, this may be done before retroverting the uterus. All hemor-](https://iiif.wellcomecollection.org/image/b2122528x_0163.jp2/full/800%2C/0/default.jpg)