Surgery : its theory and practice / by William Johnson Walsham.
- William Walsham
- Date:
- 1897
Licence: Public Domain Mark
Credit: Surgery : its theory and practice / by William Johnson Walsham. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
832/898 page 816
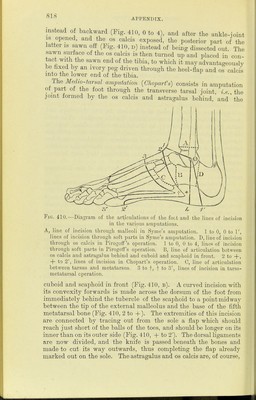
![NIG APPENDIX. The thumh&tthe carpo-metacarpa] joint may be amputated by transfcxion or by an oval incision. In the transfixion method the l-nint of the knife in operating on the light side is entered at the web of skm between the first and second metacarpal bones and made to emerge on the palmar aspect of the carpometacarpal joint. A palmar flap is then cut from the tissues forming the ball of the thumb, and the knife drawn obliquely across the back of the thumb from one extremity of the flap to the other. In operat- ing on the left side, the oblique incision across the back of the thumb is first made, then the point of the knife is thrust down through the web and made to transfix as on the right side. In the oval or circular method, the knife is entered midway between the base of the metacarpal bone and the styloid process of the radius, and the incision carried obliquely along the dorsum of the meta- carpal bone to the first phalanx, and then round the palmar surface and back again to the former incision. The fingers may be amputated by double flaps or by a long anterior flap. In amputating a finger it should be remembered that the joint is in front of the knuckle. If the whole finger requires removal, the head of the metacarpal bone should be nipped off with bone forceps, unless breadth and strength of hand is the chief desideratum, when it should be left. Amputation at the hip-joint may be done by transfixion or by Furneaux Jordan's method. Although the former can be performed with greater celerity, the latter is by far the better operation, as it is attended with less haemorrhage and provides a much more useful stump. In the transfixion method a long anterior flap is made by transfixion and cutting towards the surface. The knife is entered midway between the anterior superior iliac spine and the great trochanter, and is made to emerge as near to the tuberosity of the ischium as possible. A flap about ten inches long is then cut, the vessels being seized by the fingers of an assistant, who grasps them with the flap and turns it upwards. The limb is then everted and extended by an assistant, the joint opened, the head of the bone and great trochanter freed from their connections, and the knife carried straight out posteriorly. Haemorrhage should be controlled by Davy's lever in the rectum, or by Lister's abdominal tourniquet. In Furneaux Jordan's method, Esmarch's cord tourniquet having been applied, a circular amputation is first done through the upper third of the thigh, and all the vessels secured. The tourniquet is then removed, and an incision carried up the outer side of the thigh to the great trochanter, the soft parts with the periosteum separated from the bone, the joint opened and the disarticulation completed by freeing the remaining connections with the knife kept close to the bone. Amputation through the knee is perhaps best done by lateral flaps](https://iiif.wellcomecollection.org/image/b21514392_0832.jp2/full/800%2C/0/default.jpg)