Primary sarcoma of the peritoneum / by J.M. Elder.
- Elder, John Munro, 1859-
- Date:
- 1908
Licence: In copyright
Credit: Primary sarcoma of the peritoneum / by J.M. Elder. Source: Wellcome Collection.
Provider: This material has been provided by The Royal College of Surgeons of England. The original may be consulted at The Royal College of Surgeons of England.
2/12 page 850
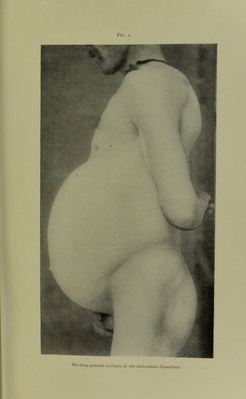
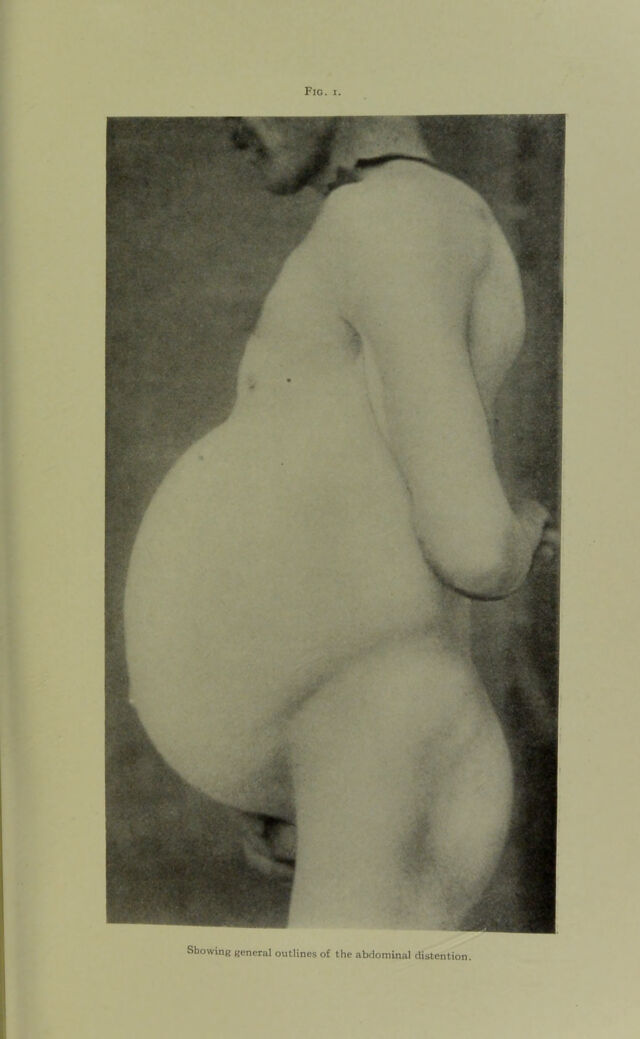
![side are markedly distended and run up to anastomose with the mammary veins. On palpation, the walls are tense but there is no rigidity on deep pressure, except over the right upper quadrant where the resistance is definitely increased but no distinct mass can be felt; no tenderness, no fluctuation. Percussion shows a marked dull note all over the anterior aspect of the abdomen except the epigastrium and flanks, where note is tympanitic. These dull and tympanitic areas are not affected by change of posture. Liver dulness begins at sixth rib in nipple line and is continuous below with dulness noted above. No change in spleen could be made out. Urine normal except trace of bile pigment. On June 25 an exploring needle was introduced into the dull area below the umbilicus and only about I c.c. of bloody serum could be obtained. This fluid showed microscopically numerous large round cells, several spindle-cells and numerous blood-cells. The temperature runs from 99j4° to normal, and pulse about 90. [The above is an extract from Dr. Lafleur’s clinical notes of the case. At this stage the patient was transferred to the surgical ward for exploratory laparotomy.] Extract from Surgical Notes.—The following questions regarding the diagnosis suggested themselves to us for solution at the exploratory laparotomy: (i) diffuse tuberculous peri- tonitis; (2) cirrhosis of the liver, with ascites; (3) omental cysts (malignant?); (4) hyatid disease, and (5) mesenteric sarcoma. We were rather inclined to regard the trouble as tuber- cular, and on June 27, under ether narcosis, which caused marked cyanosis, an exploratory incision was made in the median line below the umbilicus. On opening the peritoneum several small gelatinous cysts popped out, some of which were sent to the pathologist for examination. There was no free fluid. The tumor was seen to be chiefly in the great omentum which was adherent to the parietal peritoneum. Upon tearing through the omentum the mesentery was also seen to be in- volved. The whole omentum was filled with these cyst-like bodies, which appeared to be caught in a very vascular stroma.](https://iiif.wellcomecollection.org/image/b22419688_0004.jp2/full/800%2C/0/default.jpg)