Obstetric operations : including the treatment of hmorrhage / by Robert Barnes ; with additions, by Benjamin F. Dawson.
- Robert Barnes
- Date:
- 1870
Licence: Public Domain Mark
Credit: Obstetric operations : including the treatment of hmorrhage / by Robert Barnes ; with additions, by Benjamin F. Dawson. Source: Wellcome Collection.
Provider: This material has been provided by the Francis A. Countway Library of Medicine, through the Medical Heritage Library. The original may be consulted at the Francis A. Countway Library of Medicine, Harvard Medical School.
76/504 page 62
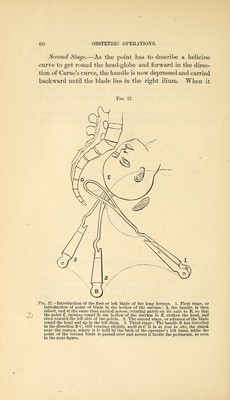
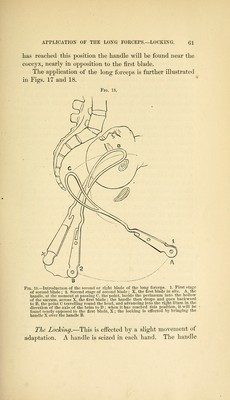
![of tlie first blade is brought a little forward over the handle of the second blade. If one blade is a little deeper in the pelvis than the other, it is either brought out, or the other is carried in until the lock is adjusted. This is commonly facilitated by pressing both handles backward against the coccyx. This movement, by throwing the blades well into the ilia, where there is room, allows the handles to be rotated a little, so as to fall into accurate relation. Accurate locking is generally evidence that the blades are properly adjusted to the head, and that the pelvis admits of the successful use of the instrument. On the other hand, their not locking is proof of their not being properly intro- duced, or of the pelvis not admitting of their a])j)lication. In the first case, that of improper introduction, the failure is generally due to neglect in passing the blades exactly in the same diameter of the pelvis—that is, in passing the sec- ond blade exactly opposite to the first^ so that if the first blade is applied in the left ilium, opposite one end of the transverse diameter, the right does not lie at the opposite end of that diameter. To remedy this error, the blade must be partly or wholly withdrawn and readjusted. In the second case, that of pelvic unfitness, the locking is prevented by the projecting promontory or other deform- ity, so distorting the pelvic diameters that the two blades cannot find room to lie in the same diameter opposite to each other. It will commonly be found that the blades will pass one on each side of the promontory, the inside of the blade not looking toward its fellow, but toward the opposite foramen ovale, where you cannot get a blade to lie. When you find this happen, you must give up the attempt to use the forceps. Pass the hand into the pelvis, if necessary; explore its dimensions and form carefully; and determine between turning and craniotomy. A correlative proposition may here be stated : Wherever the long forceps loill lock without force^ it wiay he reasonably conchided that the case is a fit one for the trial of this instrument ^ and a reason-](https://iiif.wellcomecollection.org/image/b21039914_0076.jp2/full/800%2C/0/default.jpg)



 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image