The principles and practice of surgery / by John Ashhurst ; illustrated with five hundred and thirty-three engravings on wood.
- John Ashhurst
- Date:
- 1871
Licence: Public Domain Mark
Credit: The principles and practice of surgery / by John Ashhurst ; illustrated with five hundred and thirty-three engravings on wood. Source: Wellcome Collection.
Provider: This material has been provided by the Francis A. Countway Library of Medicine, through the Medical Heritage Library. The original may be consulted at the Francis A. Countway Library of Medicine, Harvard Medical School.
129/1052 page 127
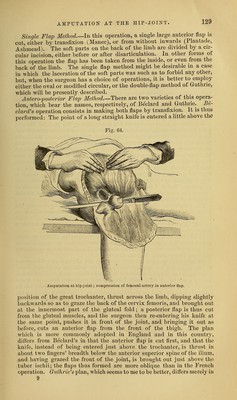
![the antero-superior edge of the condyloid cartilage, and the cartilagin- ous surface of the patella is removed by means of a small saw. Ani])utation at the Lower Third of the thigh may be conveniently done by the ordinary double-flap operation. Mr. Erichsen recommends Ver- male's operation, or that by lateral flaps, for this situation, and I doubt not that an excellent stump may be obtained by this method. The operation, however, which I have always practised myself in amputating at the lower third of the thigh, is the antero-posterior flap method, and I have found it perfectly satisfactory. The anterior flap is cut flrst, from without inwards, and should be about four inches in length, extending to the upper edge of the patella ; it should be rather square in shape, with the corners rounded off, and should embrace all the tissues down to the bone. The posterior flap, which contains the main artery, is made by transfixion, and should be about the same length as the other, thus allowing for the inevitable retraction of the muscles at the back of the thigh. Both flaps are then turned back, when a circular sweep of the knife clears the bone for the application of the saw. When the flaps are adjusted, it will be found that the bone is well covered by the front flap, and the resulting cicatrix is drawn entirely behind the line of pres- sure. Seven or eight vessels usually require ligature, though, if the case be one of chronic joint disease, the number may be larger. Amputation at the Middle or Upper Third of the thigh, if the limb be not too muscular, may be done in the same way, by antero-posterior flaps, one or both made by transfixion, according to circumstances. But if the limb be a large one, a better stump can be made by resorting to the modified circular opei'ation, as practised by Syme and Liston, making short skin flaps, and dividing the muscles at a higher point by a circular incision (see Fig. 42). The posterior muscles of the thigh always re- tract more than the anterior, and should therefore be cut rather longer. In amputating at the upper portion of the thigh, there is scarcely room for the application of a tourniquet, and the surgeon therefore commonly has to rely upon manual compression of the femoral arter}^, as it passes over the brim of the pelvis, though in some cases the aortic tourniquet might perhaps be advantageously employed. If manual pressure be resorted to, the assistant who has charge of this department should grasp the great trochanter with the fingers of the hand corresponding to the limb to be removed, and press firmly on the artery as it emerges from beneath Poupart's ligament with the thumb of the same hand; the opposite thumb is superimposed to assist and regulate the pressure, and to pre- vent any risk of slipping. In cases of injury, the form and extent of the laceration will often compel the surgeon to make irregular flaps, and to cover his stump as best he may under the circumstances. Oblique flaps may be employed in such a case, or a single long flap from any part of the thigh; it is more important to make the amputation at as low a point as possible, than to follow any one or other particular mode of operating. Amputation through the Trochanters may be occasionally required in cases of injury, or of malignant tumor involving the lower part of the femur. It is a procedure of less risk than exarticulation of the whole limb, and, in cases of malignant disease, appears to be no more likel}' to be followed by a return of the affection, than the graver operation. It is, moreover, very easy to convert this amputation into a disarticulation, by dissecting out the head and neck of the femur, if these parts be found to be diseased.](https://iiif.wellcomecollection.org/image/b21039094_0129.jp2/full/800%2C/0/default.jpg)