Imperative surgery : for the general practitioner, the specialist and the recent graduate / by Howard Lilienthal.
- Lilienthal, Howard, 1861-1946.
- Date:
- 1900
Licence: In copyright
Credit: Imperative surgery : for the general practitioner, the specialist and the recent graduate / by Howard Lilienthal. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
405/440 (page 383)
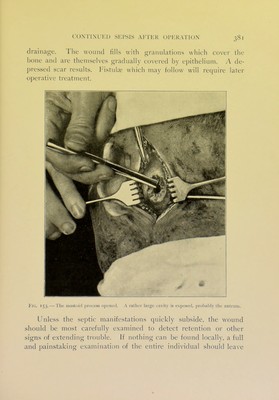
![It lies just beneath the skin, crossing diagonally the middle third of the sterno-cleido-mastoid muscle. The deep jugular vein will be found just behind and to the outer side of the common carotid, and when in a normal condition is easily recognized by its bluish hue. The head of the patient should be occasionally raised so as slightly to Hex the neck, thus permitting the vein to fill and become more easily visible. When the tissues of the neck are stretched, the vessel may become empty and flattened, so that it resembles a piece of fascia. If there is thrombosis of the sinus, the jugular will usual])' be found but partly filled or, in case the clot ex- tends rather far down, it may be entirely empty and not easv to recognize. Besides, when the disease has involved the vein in the inflammatory process, its walls may have become much thick- ened and adherent to the surrounding tissues. The part near the clavicle is apt to be the most normal in appearance. Holding this portion of the jugular carefully with an anatomical-forceps,— not a mousetooth-forceps, which might lacerate its walls, — a Mat probe may be slowly and cautiously pushed between vein and ar- tery, at the same time being sure not to include the pneumogastric nerve, which lies between and behind these vessels. A strong but thin piece of catgut should be made fast to the probe, drawn around the vein and tied securely with a surgeon's knot. The precaution of tying the jugular is intended to prevent the entrance of septic matter which may be loosened from the thrombus during the chis- elling and other manipulation. Laying a temporary packing upon the wound of the neck, a two-inch incision straight backward from the middle of the original wound of the mastoid region should be made, the scalp being clamped as before to check hemorrhage. After peeling away the pericranium, the whole wound should be held apart with sharp retractors, and the bone chiselled away as far as the inner table, beginning at the opening in the mastoid and working backward. It is best not to remove any portion of the inner table until it has been exposed over an area about an inch in length and three-quarters of an inch in width.](https://iiif.wellcomecollection.org/image/b21536351_0405.jp2/full/800%2C/0/default.jpg)