An American text-book of surgery : for practitioners and students / By Phineas S. Conner, M.D., Frederic S. Dennis, M.D., William W. Keen, M.D., Charles B. Nancrede, M.D., Roswell Park, M.D., Lewis S. Pilcher, M.D., Nicholas Senn, M.D., Francis J. Shepherd, M.D., Lewis A. Stimson, M.D., J. Collins Warren, M.D., and J. William White, M.D. Ed. by William W. Keen and J. William White.
- William Williams Keen
- Date:
- 1899
Licence: Public Domain Mark
Credit: An American text-book of surgery : for practitioners and students / By Phineas S. Conner, M.D., Frederic S. Dennis, M.D., William W. Keen, M.D., Charles B. Nancrede, M.D., Roswell Park, M.D., Lewis S. Pilcher, M.D., Nicholas Senn, M.D., Francis J. Shepherd, M.D., Lewis A. Stimson, M.D., J. Collins Warren, M.D., and J. William White, M.D. Ed. by William W. Keen and J. William White. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
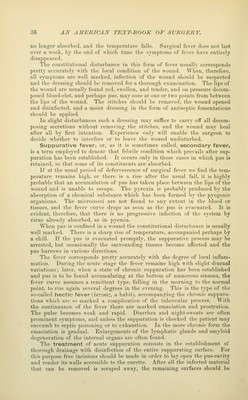
![no longer absorbed, and the temperature falls. Surgical fever does not last over a week, by the end of uhich time the symptoms of fever liave entirely disappeared. ihe constitutional disturbance in this form of fever usually corresponds pretty accurately with the local condition of the wound. Wlien, therefore, all symi)toms are well marked, infection of the Avound siiould be suspected and the dressing should be removed for a thorough examination. The lips of the wound are usually found red, swollen, and tender, and on pressure decom- posed blood-clot, and perhaps pus, may ooze at one or two points from between the lips of the wound. The stitches should be removed, the wound opened and disinfected, and a moist dressing in the form of antiseptic fomentations should be applied. In slight disturbances such a dressing may suffice to carry off all decom- posing secretions without removing the stitches, and the wound may heal after all by first intention. Experience only will enable the surgeon to decide whether to interfere or to leave the wound undisturbed. Suppurative fever, or, as it is sometimes called, secondary fever, is a term employed to denote that febrile condition which prevails after sup- puration has been established. It occurs only in those cases in which pus is retained, so that some of its constituents are absorbed. If at the usual period of defervescence of surgical fever we find the tem- perature remains high, or there is a rise after the usual fall, it is highly probable that an accumulation of pus has taken place between the lips of the wound and is unable to escape. The pyrexia is probably produced by the absorption of a chemical substance which has been formed by the pyogenic organisms. The micrococci are not found to any extent in the blood or tissues, and the fever curve drops as soon as the pus is evacuated. It is evident, therefore, that there is no progressive infection of the system by virus already absorbed, as in pj^emia. When pus is confined in a wound the constitutional disturbance is usually well marked. There is a sharp rise of temperature, accompanied perhaps by a chill. If the pus is evacuated promptly, the suppurative process may be arrested, but occasionally the surrounding tissues become affected and the pus burrows in various directions. The fever corresponds pretty accurately Avith the degree of local inflam- mation. During the acute stage the fever remains high with slight diurnal variations; later, when a state of chronic suppuration has been established and pus is to be found accumulating at the bottom of numerous sinuses, the fever curve assumes a remittent type, falling in the morning to the normal point, to rise again several degrees in the evening. This is the type of the so-called hectic fever (Ixr^zor, a habit), accompanying the chronic suppura- tions Avhich are so marked a complication of the tubercular process. ^^ ith the continuance of the fever there are marked emaciation and prostration. The pulse becomes weak and rapid. Diarrliea and night-sweats are often prominent symptoms, and unless the sup])uration is checked the patient may succumb to septic poisoning or to exhaustion. In the more chronic form the emaciation is gradual. Enlargements of the lymphatic glands and amyloid degeneration of the internal organs are often found. The treatment of acute suppuration consists in the establishment of thorough drainage with disinfection of the entire suppurating surface. For this purpose free incisions should be made in order to lay open the pus-cavity and render its walls accessible to the curette. After all the infected material that can be removed is scraped away, the remaining surfaces should be](https://iiif.wellcomecollection.org/image/b21217014_0070.jp2/full/800%2C/0/default.jpg)