Licence: Public Domain Mark
Credit: Surgical operations / by Sir William MacCormac. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
57/160 page 41
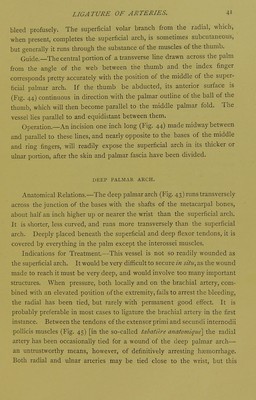
![bleed profusely. The superficial volar branch from the radial, which, when present, completes the superficial arch, is sometimes subcutaneous, but generally it runs through the substance of the muscles of the thumb. Guide.—The central portion of a transverse line drawn across the palm from the angle of the web between the thumb and the index finger corresponds pretty accurately with the position of the middle of the super- ficial palmar arch. If the thumb be abducted, its anterior surface is (Fig. 44) continuous in direction with the palmar oudine of the ball of the thumb, which will then become parallel to the middle palmar fold. The vessel lies parallel to and equidistant between them. Operation.—An incision one inch long (Fig. 44) made midway between and parallel to these lines, and nearly opposite to the bases of the middle and ring fingers, will readily expose the superficial arch in its thicker or ulnar portion, after the skin and palmar fascia have been divided. DEEP PALMAR ARCH. Anatomical Relations.—The deep palmar arch (Fig. 43) runs transversely across the junction of the bases with the shafts of the metacarpal bones, about half an inch higher up or nearer the wrist than the superficial arch. It is shorter, less curved, and runs more transversely than the superficial arch. Deeply placed beneath the superficial and deep flexor tendons, it is covered by everything in the palm except the interossei muscles. Indications for Treatment.—This vessel is not so readily wounded as the superficial arch. It would be very difficult to secure z« situ^ as the wound made to reach it must be very deep, and would involve too many important structures. When pressure, both locally and on the brachial artery, com- bined with an elevated position of the extremity, fails to arrest the bleeding, the radial has been tied, but rarely with permanent good effect. It is probably preferable in most cases to ligature the brachial artery in the first instance. Between the tendons of the extensor primi and secundi internodii poUicis muscles (Fig. 45) [in the so-called tabatih-e anatoviique] the radial artery has been occasionally tied for a wound of the deep palmar arch— an untrustworthy means, however, of definitively arresting haemorrhage. Both radial and ulnar arreries may be tied close to the wrist, but this](https://iiif.wellcomecollection.org/image/b21979431_0057.jp2/full/800%2C/0/default.jpg)