A surgical handbook : for the use of students, practitioners, house-surgeons, and dressers / by Francis M. Caird and Charles W. Cathcart.
- Caird, Francis Mitchell, 1853-1926
- Date:
- 1889
Licence: Public Domain Mark
Credit: A surgical handbook : for the use of students, practitioners, house-surgeons, and dressers / by Francis M. Caird and Charles W. Cathcart. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
22/290 (page 8)
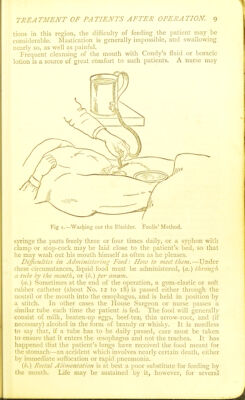
![with thirst, water or milk anil water may be administered per anum instead of by the mouth. After flatus has been passed, as it usually is twenty or twenty-four hours after the operation, the diet is gradually improved, beginning with milk and water. Nutrient enemala may sometimes be recpiircd, should tendency to vomiting continue (see p. lo). {d.) Opcnilifliis f/^///f Genilo-Urinary Tract.—The chief point to be attended to in the after-treatment of ])atients whose genito- urinary tract has been operated upon, is to diminish the acidity of the urine and lessen the work of the kidney by keeping down the albuminoid clement in the food. A diet, consisting chiefly of milk and starchy foods, is best for this purpose. When the kidney has been injured, the bowels must be kept open. Frxtid urine may be improved by the free administration by the mouth of boracic acid oz. sat. solution every three hours), sul]jho-carbolate of soda (20 grs. every two hours), naphthalin, and probably also by sandal- wood oil and copaiba, as well as by the injection of weak antiseptics into the bladder. IVasliiiig out the Bladder is often of great service when the urine is putrid, and the mucous membrane unhealthy. Some surgeons use a double-way catheter. With this instrument, fluid is injecteil by one of the channels, while it flows out by the otlier; but as the mucous membrane is not thus distended and its folds exposed to the fluid, we prefer the ordinary single-way catheter. The fluids at flrst used must lie warm (80 to 100° F.) and unirritating antiseptics—<?.,(,■•., 1-4000 corrosive sublimate lotion, half strengtli boracic lotion, or 1-200 carbolic acid; (|uinine2-3 grains per ounce, with I min. dilute suljihuric acid ])er grain; iodoform 2-4 grains per ounc-e, with a little mucilage to suspend it {Tiriclisen). When the urine is no longer septic, astringent injections may be required—acetate of lead, ^ gfain to g' (in urine alkaline and dejiositing phosphates, 7'hoiiison) ; nitrate of silver, ){ to ^4 grain to oi > tannin, i grain to gi- The quantity of fluid injected must depend on the state of the patient's bladder—as much as can be liorne without much inconveni- ence. Sir Henry Thomson limits the amount to 2 ounces. A catheter (soft for preference) is passed into the bladder, and the urine drawn off. The selected fluid is then injected with a syringe (Higginson's ball or ordinary piston s)'ringe), or is allowed (Ijy syphon or water-head, see p. 9) to flow in from a height of i or 2 feet at most. It is then allowed to escape, and is probably at first turbid ; the process is repeated until the returning fluid is clear. Foulis has introduced a simple and cheap apparatus for washing out the bladder (Fig. i). He attaches a stopcock to the lower part of a common-handled mug, holding a pint. From the stopcock he leads an india-rubber tube to the catheter, to the end of which he fixes a T-tube. In washing out the bladder he has only alternately to open and close the end of the T-tube, and fluid will enter or leave Ih.e bladder as desired. (e.) Ofierations on the Mouth or Jaws.—After extensive opera-](https://iiif.wellcomecollection.org/image/b21514124_0022.jp2/full/800%2C/0/default.jpg)