A surgical handbook : for the use of students, practitioners, house-surgeons, and dressers / by Francis M. Caird and Charles W. Cathcart.
- Caird, Francis Mitchell, 1853-1926
- Date:
- 1889
Licence: Public Domain Mark
Credit: A surgical handbook : for the use of students, practitioners, house-surgeons, and dressers / by Francis M. Caird and Charles W. Cathcart. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
246/290 (page 234)
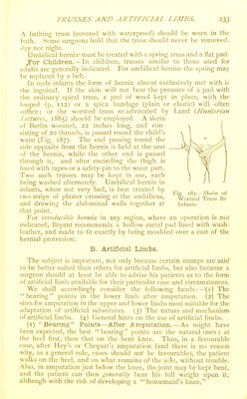
![After these come amputations in wliich the skin of the iieel ami that or the front of the knee, respectively, are folded over the sawn surface of the correspondint^ articular end of the adjacent hone. Thus, in most, but not in all, ol Syme's amputations, the full weight can be borne on the face of the stump. In a ('arden's or Gritti's a certain but variable amount of the weight only can be borne. Ne.xt in order of bearing power W(juld come amputations through the same articular enils of the femur or tibia, but where the covering skin had, from the nature of the case, to be taken from the lateral or flexor aspects of the limb. When the shaft, instead of the (lower) articular end of the femur or tibia, is sawn through, little, if any, bearing can ever be taken on the resulting stump, however favourable in other respects the amputation may be. h'ortunately, however, the instrument-maker has other points of bearing to depend on besides the face or end of the stum]). Below the knee a considerable part, if not the whole, of the patient's weight can often be borne on the upper ends of the libia and fibula. Above the knee a considerable proportion can be borne on the muscles of the thigh by means of a lacing shield, and there are few cases where, if need be, the wliole weight cannot be borne on the tuber-ischii and trochanter, by the adjustment of a pailded ring like that used for Thomas's knee-s|)lint (p. 189). The lower in the limb the bearing can be taken, the greater the advantage to the patient in walking. The instrument-maker retjuires to adapt his points of bearing to the [)articular case, sometimes (lislributing the weight over several parts, sometimes conlining it to one. (2) Sites for Amputation.—{a.) In the upper limb there is no question that above the Angers (see p. 92) the greater the length of the natural parts left—other things being ctjual—the better for the patient in every way. Artificial i)arts, more or less efficient, can always be adapted to the stumjjs. The surgeon's way is, therefore, clear—he must leave as much as he can. {b.) As regards llu: lower limb there is much greater difference of opinion. Some instrument-makers go so far as to say that a jump is to be made from the ball of the toes to the level of a Syme or i'irogoff, and that if 4 inches below the knee cannot be left to allow of a strong control of the artificial limb by the stump, the surgeon should amputate 4 inches al)ove the knee to give room for the mechanism of an artificial knee-joint. From these views we entirely dissent.* After a careful examination of the whole subject, our conclusion is that the surgeon should take the least sacrifice of parts as his guide, and amputate as low as the circumstances of the case permit. He should spare as much bone as he can, and he may be satisfied that artificial limbs can be made for the stumps. The longer the limb left, the better the walking power. (3) Artificial Limbs.—We cannot, of course, attempt more here than a discussion of general principles :— ^ (a.) For Partial Amputations of tlie. Foot (Key's or Chopart s), * See Ed. Medical Jouriial^ March, 1888, and i38g.](https://iiif.wellcomecollection.org/image/b21514124_0246.jp2/full/800%2C/0/default.jpg)