Lectures on nervous diseases from the standpoint of cerebral and spinal localization, and the later methods employed in the diagnosis and treatment of these affections / by Ambrose L. Ranney.
- Date:
- 1888
Licence: Public Domain Mark
Credit: Lectures on nervous diseases from the standpoint of cerebral and spinal localization, and the later methods employed in the diagnosis and treatment of these affections / by Ambrose L. Ranney. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
99/812 page 75
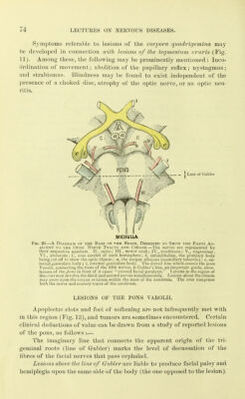
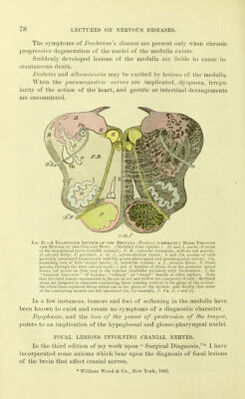
![Lesions below the line of Gubler produce crossed paralysis of the seventh nerve and body type, the face being paralj'zed upon the same side as the lesion, while a hemiplegia is developed upon the opposed side of the body. The trigeminus nerve may be paralj'zed by lesions of the pons, if it lies within the inner two-thirds of the reticular formation (according to the researches of Starr). If siicli a lesion be situated high up in the pons, trigeminal paralysis will co-exist with a hemianaesthesia of the opposed half of the body; if situated low in the pons, the trigeminal paralysis and the hemianaesthesia will be upon the same side. The point of union of the ascending and descending roots of the fifth nerve is nearly at the level at which the fifth nerve escapes from the pons (line of Gubler). Difficulties of articulation may often be considered as diagnostic of lesions of the pons or medulla, provided the presence of aphasia of cerebral origin can be excluded by the history of the case. There is unquestionably a tract of fibres (the motor speech tract) that serves to connect the centres in the medulla with the cortical centres for the move- ments of the face and tongue. Conjugate deviation of the eyes may accompany a lesion of the pons. This symptom is not pathognomonic, however, because it may occur also with cortical lesions of the cerebrum and lesions of the internal capsule. The motor, sensory, and vaso-motor effects of lesions within the pons are manifested in the extremities, chiefly, but not exclusively, upon the side opposed to the lesion. This is not the case with those cranial nerves whose fibres of origin probably traverse the pons (the fifth, sixth, seventh, eighth [?], eleventh [?], and twelfth). The effects of intrapon- tine disease upon some of these nerves, at least, are modified by the seat of the lesion, as has been shown in preceding paragraphs. Contraction of the pupils during an apoplectic attack is to be re- garded as strongly diagnostic of a clot within the pons. Hemorrhage into the pons is usually followed by coma and sudden death, if the clot be large or if the blood escape into the fourth ventricle. The diagnostic points mentioned above apply, therefore, more particularly to foci of softening and destructive lesions of small size and slow devel- opment. When blood escapes into the fourth ventricle, convulsions are observed, and death is liable to follow rapidl3^ Disturbances of the circulatory and respiratory functions may occur in connection with lesions of the pons ; but they are to be regarded rather as evidences that the medulla oblongata is directly implicated or sub- jected to pressure.](https://iiif.wellcomecollection.org/image/b21923346_0099.jp2/full/800%2C/0/default.jpg)

 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image