A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen.
- Wells, J. Soelberg (John Soelberg), -1879
- Date:
- 1883
Licence: Public Domain Mark
Credit: A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
113/898 page 119
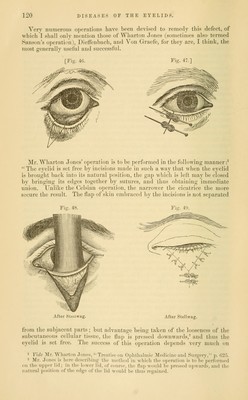
![Avhicli the palpebral aperture should be narro^A'ed. The effect which this narrowinoj has upon the edge of the everted lid should likewise be noted, as also the fact whether the lid has to be a little raised or depressed, in order to bring it into a proper position. If the puncta are erect or everted, they should be slit up, so as to facilitate the entrance of the tears into the sac. Tarsoraj)hia, which was first devised by Walther, is to be performed as follows : The operator, having inserted a horn or ivory spatula between the lids at the outer canthus, makes an incision through the skin and con- nective tissue parallel to the edge of the upper lid, and about three-quarters of a line from its margin. This incision is to be commenced at the outer canthus, and carried along the edge of the lid to a distance of from one and a half lines to three lines; it is then to be carried vertically down to, and through the anterior edge of the lid. This portion of the lid, including its cilia, is then to be completely excised from this point to the outer canthus, care being taken that the hair-follicles are not divided obliquely, but entirely removed, otherwise they will grow again. The same proceeding is then to be repeated in the lower lid, so that the two raw surfaces of the edges of the lids can be accurately applied to each other, and united by two or three sutures. In order still more to facilitate the union, and to give the lashes a more perfect and favorable inclination. Von Graefe^ has modified the opera- tion in the following manner: He carries on horizontally the inner portion of the vertical incision (which has been made perpendicularly through the edge of the lid) to the extent of about one line or one and one-half line toward the nose, along the posterior border of the margin of the lip, and pares the latter by removing a small slip of conjunctiva. This is to be done in each lid, the cilia being of course left at the outer portion of this part of the lid. In those cases in which there is a considerable elongation of the edge of the lower lid, as well as of its cartilage, an unsightly pucker or fold is apt to be produced by the sutures at the outer canthus. To obviate this, a triangular portion of the substance of the lower lid should be excised near the outer commissure, the base of the triangle being turned toward the edge of the lid. The operation of tarsoraphia will also be found very useful in lagophthalraos due to paralysis of the portio dura, as well as in that which is sometimes noticed after the old squint operation. For the senile or spastic forms of ectropium, tarsoraphia will be found greatly preferable to the operation of Adams, which consists in the removal of a triangular, V-shaped piece from the whole thickness of the lid, the base of the triangle being turned toward the margin of the latter, and the apex toward the cheek. [Fig. 46.] The edges of the wound are then to be brought accurately together by sutures, one of which should be inserted close to the margin of the tarsus, so that the lips of the wound may be brought very closely together at this point. [Fig. 47.] The chief disad- vantage of this operation is that, when it is done near the central part of the lid, it shortens the edge of the latter without elevating it at the outer canthus, hence it is closely pressed against the eyeball, which may, more- over, be somewhat irritated by the pucker or fold to which the cicatrix gives rise. If this operation is adopted, it should, therefore, be performed close to the outer canthus, as this tends to elevate the edge of the lid at this point. We have now^ to turn our attention to those cases in which a partial or complete ectropium is due to a cicatrix, which is situated at a short distance from the edge of the lid, and causes eversion of the latter by traction.](https://iiif.wellcomecollection.org/image/b20999392_0113.jp2/full/800%2C/0/default.jpg)


 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image