A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen.
- Wells, J. Soelberg (John Soelberg), -1879
- Date:
- 1883
Licence: Public Domain Mark
Credit: A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
115/898 page 121
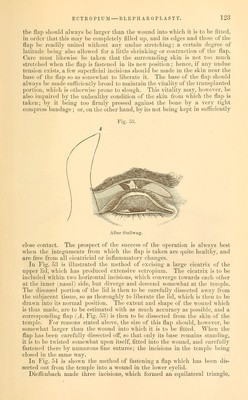
![the looseness of the cellular tissue. For some days before the operation, therefore, the skin should be moved up and down, in order to render the cellular tissue more yielding. In Figs. 48 and 49 the method of performing this operation upon the lower eyelid is illustrated. A horn spatula having been inserted beneath the lower lid, so as to render this tense, two straight incisions are to be made from the edge of the lid, in such a manner that they converge toward each other, and meet at such a distance below the lid, that the cicatrix is com- pletely included within the triangular flap thus formed. The flap is then to be pressed upwards, so as to bring the edge of the lid into its normal position, and all the opposing bridles of cellular tissue are to be divided, Avithout, however, dissecting off the flap from the subjacent parts, except, perhaps, very slightly at the periphery. The edges of the wound existing below the apex of the flap are next to be closely united by two common or twisted sutures ^Fig. 49), and then the two edges of the flap are to be accu- rately united by sutures at each side to the opposite margin of the wound. If it be necessary somewhat to shorten the edge of the lid, tarsoraphia may be united with this operation. The above method of operating is especially indicated in those cases of ectropium in which the shape and form of the lid are but little changed, its margin being chiefly elongated. Dieffenbach devised the following operation for eversion of the low^er lid, due to a cicatrix situated at a short distance from it. The cicatrix is to be included within a triangular flap, the base of which [Fig. 50, c c] is to be turned towai'ds the margin of the lid, the apex to the cheek. This triangular portion is then to be removed, and the incision, which represents the base of the triangle, is to be prolonged horizontally on each side to a short distance [a], in order to facilitate the approximation of the lateral edges [b b'] of the triangle, which should be raised from the subjacent parts by a few incisions with the scalpel. The two lateral incisions of the triangle are to be united by fine sutures, and then the horizontal incision, on each side of the base of the triangle, is also to be brought together by sutures [as is represented in Fig. 51]. Von Graefe has lately introduced the following method of operating for the severer cases of ectropium of the lower lid, more especially those which are the result of chronic blepharo-adenitis. He makes a horizontal incision just behind the edge of the lid, in the intermarginal space, from the lower punctum to the outer canthus. From the extremities of this line (Fig. 52), two incisions are then to descend vertically down the cheek, for a distance of from eight lines to ten lines. The square flap A is next to be dissected up, and, if necessary, somewhat raised subcutaneously beyond the lower extremi-](https://iiif.wellcomecollection.org/image/b20999392_0115.jp2/full/800%2C/0/default.jpg)





 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image