A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen.
- Wells, J. Soelberg (John Soelberg), -1879
- Date:
- 1883
Licence: Public Domain Mark
Credit: A treatise on the diseases of the eye / By J. Soelberg Wells... Together with selections from the test-types of Prof. E. Jaeger and Prof. H. Snellen. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
119/898 page 125
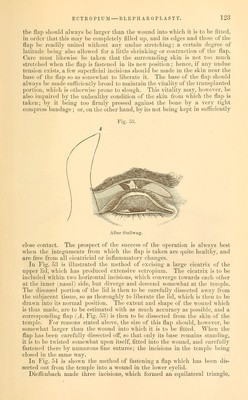
![the new flap should then be made somewhat longer, so that this portion of the flap may form the edge of the lid. KnajDp has described' an ingenious modification of blepharoplasty, per- formed by him in a case in which a cancerous tumor occupied the inner two- thirds of the lower lid (including its edge), extending somewhat beyond the inner angle of the eye, and involving the skin of the nose to an extent of from two lines to three lines. As the flap is apt to contract when it is made with its base downwards, and may thus give rise to ectropium. Dr. Knapp, at the suggestion of Dr. Fritz Pagenstecher, operated in the following manner : He included the tumor between straight incisions (which were carried well into the healthy tissue). After the morbid growth had been thoroughly removed, he prolonged the internal horizontal incisions towards the nose, and thus prepared a square, horizontal flap at this point. He then made (in the prolongation of the palpebral aperture) an incision from the outer canthus slightly upwards into the skin of the temple; and next a second incision, which was at first a straight prolongation of the lower edge of the wound, but was then somewhat arched downwards on to the cheek, the con- cavity looking downwards. The long flap thus formed, and which increased considerably in width towards its base, was then dissected off from the sub- jacent tissue, drawn forwards, and its inner angles united by twisted sutures to the vertical edge of the nasal f^ap. Both flaps, though tightly stretched, entirely covered the wound, and formed a very successful artificial lid. The external fourth of the latter, which had remained standing, now formed the most internal portion. The edges of the wound were then carefully united by very numerous sutures, and a compress bandage applied for forty-eight hours. Perfect union resulted, and the patient was discharged fourteen days afterwards, completely cured. The palpebral aperture was slightly (about two lines) diminished in length, but could be easily and perfectly opened and closed by the action of the upper lid. The lower lid was closely applied to the globe, and Knapp states that this was one of the most successful cases of blepharoplasty with which he has met. [Knapp^ has since operated by the same method upon similar cases, and the result left nothing to be desired. But, although this method produces very excellent results, it is limited in its eflSciency, and Knapp has not ventured by its means to repair the loss of more than three-quarters of the lower lid.—H.] In cases in which we unite the opposite edges of two flaps, care must always be taken to allow a suflicient amount of skin, so as to permit a certain degree of contraction and gaping of the edges of the flaps, in case they should not unite by first inten- tion, which is not unlikely to occur. In those cases in which cicatrices or cancerous growths implicate the inner or outer canthus, and to a small extent the opposite edges of the two lips, the flap w'hich is to cover the wound may be taken from the skin of the nose or the temple, according to the situation of the disease. In such instances, the following operation, devised by Hasner, will be found useful: If the morbid growth be situated at the outer canthus, and implicates to a certain extent the edges of the upper and lower lid, the tumor is to be included above and below between elliptical incisions, which should be laid well in the healthy integument. The line of junction of these two incisions should then be slightly prolonged outwards, and a sufficiently large flap be excised from the temple. The upper extremity of this flap is to be bifurcated, so as to fit easily into the wound made in the edges of the lid at the outer canthus. If the disease is situated at the inner canthus, the flaj) should be taken from the side of the nose. 1 A. f. 0., xiii. 1, 183. p Arcliiv of Ophthal. andOtoL, vol. ii. p. 209.]](https://iiif.wellcomecollection.org/image/b20999392_0119.jp2/full/800%2C/0/default.jpg)





 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image