The surgery of oral diseases and malformations : their diagnosis and treatment / by George Van Ingen Brown.
- Brown, George van Ingen, 1861-1948.
- Date:
- 1912
Licence: In copyright
Credit: The surgery of oral diseases and malformations : their diagnosis and treatment / by George Van Ingen Brown. Source: Wellcome Collection.
749/792 (page 703)
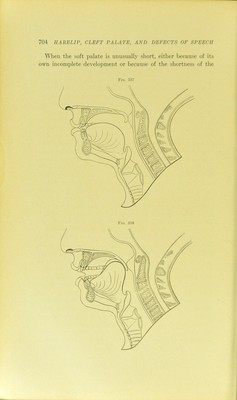
![The Correction of Anatomical Defects.—This has already been pro\dded for in the description of the prevention and correction of nasal, palatal, lingual, maxillary, and other oral malformations; with the single exception of the operative treatment of cases having defective speech from imperfectly developed palates, that are not cleft, and which upon casual examination give no evidence of the imperfection. These palates have been from time to time referred to in the discussion of other divisions of the subject. The author’s method of treatment is based upon the belief that when there is no nerve lesion or congenital motor insufficiency in the control of the movements of the soft palate, the reason why there is wrong escape of air through the nose, with an imperfect sound such as that which is characteristic of cleft palate cases, is because it is impossible for such patients perfectly to approxi- mate the posterior wall of the pharjmx and the soft palate at the proper moment, as is shown in Fig. 357, which illustrates the contact of the velum with the projection in the pharynx formed by the pharyngoconstrictor muscles whereby closure of the nasal openings takes place. This occurs with slight variations in the pronunciation of the elementary vowel sounds and the consonants p, b, t, d, V, s, z, c, h, j, th, r, sh, 1. Fig. 358 shows the impact of the tongue against the soft palate required in k, g, and ng.^ Kingsley’s palatograms (Fig. 359) indicate the points of contact of the tongue and palate in articulation of speech sounds. Obviously, if the hard palate is short, the levator and tensor palati muscles will not have the same leverage as would be the case with a perfect outline at the jjosterior border of the hard palate. ^Moreover, the angle at which the velum is suspended will be such as to make it necessary for it to be carried farther upward and backward in order to complete physiological speech function in relation to the pharyngeal wall. More is therefore required of muscular action that is necessarily deficient. The difficulty is still further increased because the natural effect of this condition upon the jjalatoglossi muscles is to cause them to be shorter than would be expected if their an- tagonists of the velum were oi)erating from i)oints of attachment farther back, as would be the case with a normal hard ])alate. ' American System of Dentistry.](https://iiif.wellcomecollection.org/image/b28101789_0749.jp2/full/800%2C/0/default.jpg)