International clinic week at the New York Polyclinic Medical School and Hospital during the International Surgical Congress, April, 1914 / by Alfred C. Jordan [and others].
- Date:
- 1914
Licence: In copyright
Credit: International clinic week at the New York Polyclinic Medical School and Hospital during the International Surgical Congress, April, 1914 / by Alfred C. Jordan [and others]. Source: Wellcome Collection.
Provider: This material has been provided by The Royal College of Surgeons of England. The original may be consulted at The Royal College of Surgeons of England.
89/106 page 87
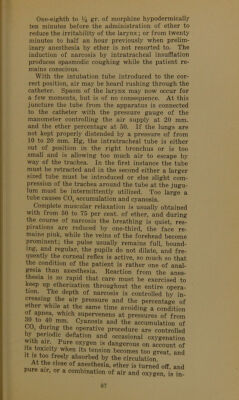
![One-eighth to % gr. of morphine hypodermically ten minutes before the administration of ether to reduce the irritability of the larynx; or from twenty minutes to half an hour previously when prelim- inary anesthesia by ether is not resorted to. The induction of narcosis by intratracheal insufflation produces spasmodic coughing while the patient re- mains conscious. With the intubation tube introduced to the cor- rect position, air may be heard rushing through the catheter. Spasm of the larynx may now occur for a few moments, but is of no consequence. At this juncture the tube from the apparatus is connected to the catheter with the pressure gauge of the manometer controlling the air supply at 20 mm. and the ether percentage at 50. If the lungs are not kept properly distended by a pressure of from 10 to 20 mm. Hg, the intratracheal tube is either out of position in the right bronchus or is too small and is allowing too much air to escape by way of the trachea. In the first instance the tube must be retracted and in the second either a larger sized tube must be introduced or else slight com- pression of the trachea around the tube at the jugu- lum must be intermittently utilized. Too large a tube causes C02 accumulation and cyanosis. Complete muscular relaxation is usually obtained with from 50 to 75 per cent, of ether, and during the course of narcosis the breathing is quiet, res- pirations are reduced by one-third, the face re- mains pink, while the veins of the forehead become prominent; the pulse usually remains full, bound- ing, and regular, the pupils do not dilate, and fre- quently the corneal reflex is active, so much so that the condition of the patient is rather one of anal- gesia than anesthesia. Reaction from the anes- thesia is so rapid that care must be exercised to keep up etherization throughout the entire opera- tion. . The depth of narcosis is controlled by in- creasing the air pressure and the percentage of ether while at the same time avoiding a condition ot apnea, which supervenens at pressures of from dO to 40 mm Cyanosis and the accumulation of bU2 during the operative procedure are controlled y penochc deflation and occasional oxygenation with air Pure oxygen is dangerous on account of its toxicity when its tension becomes too great and ]t aA? Aeely absorbed by the circulation. t the close of anesthesia, ether is turned off and Pure air, or a combination of air and oxygen, i^Tn](https://iiif.wellcomecollection.org/image/b2244807x_0091.jp2/full/800%2C/0/default.jpg)