Report of the Commissioner of Public Health / Western Australia.
- Western Australia. Public Health Department
- Date:
- [1966]
Licence: Public Domain Mark
Credit: Report of the Commissioner of Public Health / Western Australia. Source: Wellcome Collection.
128/166 (page 110)
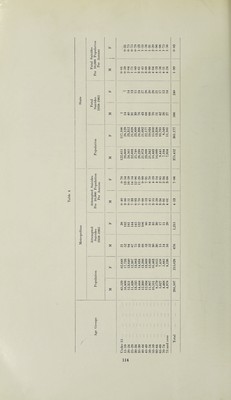
![Suicide and Self-Inflicted Injury Since 1958 Morbidity Statistics have been maintained for patients admitted to the major hospitals in metro¬ politan Perth. These statistics are recorded in an abbreviated form in an annual tabulation in the Commissioner ol Public Health’s Annual Report. This report gives a more detailed breakdown of the statistics concerned with Suicide and Self-Inflicted injury (E Code 970-979). The information regarding the unsuccessful suicides is obtained from the hospital morbidity statistics. Information regarding the successful suicides is extracted from mortality statistics in the Statistical Register. The paper deals with the consolidated statistics collected over the eight years 1958- 1965. I he programme for the extraction of data shown in the following tabulations was prepared in the depart¬ ment of the Government Statistician and the data was extracted by the computor in that Department. I able I shows that during the eight years under review 1,900 unsuccessful suicides were treated in metro¬ politan hospitals. During the same time there were 510 fatal suicides in the metropolitan area and 326 outside the metropolitan area in the rest of the State. I he pattern of suicide or suicidal attempt is cpiite different between male and female and different between metropolitan area and country. There were 681 unsuccessful attempts by males in the metropolitan area and 332 successful or fatal suicides, a ratio in the vicinity of 2 to 1. In the females the corresponding figures are 1,219 and 178, a ratio of 7 to 1. If 1 able 1 is examined in conjunction with Table II it is seen that the most prevalent form of attempted suicide is overdose of analgaesic or soporific substances with the barbiturates by far the most popular choice. Although these drugs produce the highest number of fatal suicides they are comparatively ineffectual considering flit laige number of unsuccessful attempts that are made with them. They are, however, twice as successful in men as in women. The same a]iplies to other forms of poisoning, the women being even still less successful. Where women are determined to be successful they choose domestic gas or drowning, as man chooses the exhaust from his car, hanging or gunshot, there is a tendancy too, where cutting instruments are involved, for a woman to cut her wrists and a man to cut his throat. lhe availability of the instrument for committing suicide apjiears to play a large part in its choice. As ah eady noted women use the gas oven, men the car exhaust. Country people show a preference, particularly in men, to poisons other than soporifics. Pest exterminating poisons are freely available in the coimtry. Men in the country use firearms as their favourite form of committing suicide. Phis raises the inevitable question ; does the availability of a means of suicide play any part in determining whether or not suicide takes place or does it merely determine the type of suicide. Would the countrymen have died if they liadn t had a rifle handy ; would the housewives have died if they hadn’t had a gas oven? As the populations of country and metropolitan area are roughly the same, 510 fatal suicides in the metro¬ politan area against 326 in the country indicates a greater tendency to suicide in the city. This is also suggested in the Occupational 1 able \ where suicides in Agricultural Workers and Miners are lower than in the other groups. Fable III shows the distribution by age and sex of the various methods of attempting suicides. Table IV shows these figures for the metropolitan area and the successful suicides for the State worked out to an index of unsuccessful and successful suicides per 10,000 of the population per annum and these indices are graphically displayed in the accompanying graph. From the latter we get the extraordinary picture of the high rate of self-inflicted injuries and unsuccessful suicides in the young with a rapid decline in such attempts in middle age onwards. Successful suicides on the other hand increase with age with the male peak at 65-69 and the female peak at 55-59. Successful suicide in males is more than twice as prevalent as in females but unsuccessful attempts in males are little more than half such attempts in females. The peak of unsuccessful attempts occurs in both ages in the 20-24 age group. Table V tries to illustrate the significance of occupation in attempted suicide. The attempted suicides in the \aiious occupations are shown as a percentage of the total admissions in these occupations. lable VI shows a breakdown of the occupational groups with a high incidence of attempted suicide, into male and female components to indicate the influence of the female on the total figure. The figures are unfor¬ tunately limited in their usefulness because of the non-recording of occupation in a disproportionately large number of admissions other than attempted suicide. We get the impression, however, that agricultural workers and miners are singularly free from attempted suicide, lhe exception is the extraordinary high figure for shearers. The figure here of 3.43 per cent, of admis¬ sions is the highest recorded, if two air hostesses are omitted, and is free from any female influence. As might be expected high incidence groups are groups in which young females are employed but a sig¬ nificant number of males appear in such groups as students, clerks, shopkeepers, salesmen, stonemasons and shearers, to suggest that a special suicidal tendency is associated with such occupations.](https://iiif.wellcomecollection.org/image/b31480512_0128.jp2/full/800%2C/0/default.jpg)