Obstetrics : the theory and practice ; including the diseases of pregnancy and parturition, obstetrical operations, etc. / by P. Cazeaux ; remodelled and rearranged, with additions and revisions, by S. Tarnier.
- Pierre Cazeaux
- Date:
- 1885
Licence: Public Domain Mark
Credit: Obstetrics : the theory and practice ; including the diseases of pregnancy and parturition, obstetrical operations, etc. / by P. Cazeaux ; remodelled and rearranged, with additions and revisions, by S. Tarnier. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
76/1140 (page 72)
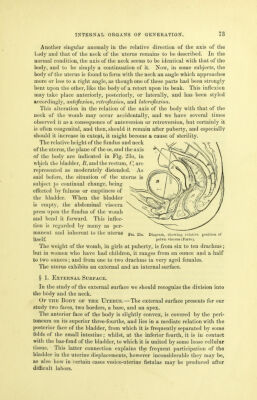
![usually on the median line, between the bladder and n cturu, being retained in position by the round and the broad ligaments on the sides, and below by the vagina, upon which it rests. [The situation of the uterus is affected by the fulness or emptiness of the bladder. When the latter is empty, the uterus is near the pubis and the neck directed back- ward. When the bladder is full, the uterus is pushed back, and its axis corresponds nearly with that of the vagina.] As we have said before, the neck of the uterus is embraced about its middle by the mucous membrane of the vagina, being thereby divided into two portions, of which the one situated above the insertion of the vagina is called the superior vaginal; and the other, which projects into the upper part of that canal, is termed the inferior vaginal portion of the neck. The connections of the uterus are very loose and extensible; it therefore exhibits a great degree of mobility, and may easily be moved in every direction. Its volume varies with age, being quite small prior to the fifteenth year, but augmenting rapidly at this era; the womb never resumes completely its pi'imitive dimensions in women who have borne children, and finally, in advanced age, it often appears to waste away, and to dwindle down to the size it had prior to the fifteenth year. Its dimensions after puberty are as follows, viz.: The vertical diameter varies from two and five-eighths to two and three-quarter inches; the transverse one, at the fundus, one and three- eighths to one and a half inches. Certain physiological conditions produce a great augmentation in its volume. For instance, I have frequently observed at the approach of the monthly courses, that it presented twice the ordinary size at least, and in some women the increase in volume is so marked at this jjeriod as to be mistaken for the commencement of a preg- nancy. (See Diagnosis of Pregnancy.) The uterus likewise varies in situation at different epochs; thus it sur- mounts the superior strait in the foetus, and rests in the abdominal cavity, so that the Fallopian tubes and ovaries occupy the iliac fossoe, the fundus uteri corresponding to the fifth lumbar vertebra. After birth, in conse- quence of the development of the pelvis, it appears to sink gradually into the excavation, and, at ten years, the fundus is on a level with the superior strait, but subsequently gets below this point. The womb is generally inclined to the right or left in aged females, or is turned backwards on the rectum. The axis of the uterus approaches that of the inferior strait in many women, especially in those having a short vagina. It must further be observed, that the direction described by us as normal, is far from being constant in all women ; thus, in some cases, the fundus may be thrown so far forwards as to render the anterior wall the most inferior part, thereby constituting what pathologists have described as an anteversion; in others, the superior border is thrown towards the most inferior portion of the sacrum, the neck being carried behind the posterior face of the pubis, thus producing a retroversion; again, it is often turned towards one side of the excavation, the neck being directed to the opposite side: this is lateral version,.](https://iiif.wellcomecollection.org/image/b21515013_0078.jp2/full/800%2C/0/default.jpg)