Licence: Public Domain Mark
Credit: Manual of practical anatomy / by D.J. Cunningham. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
593/726 (page 561)
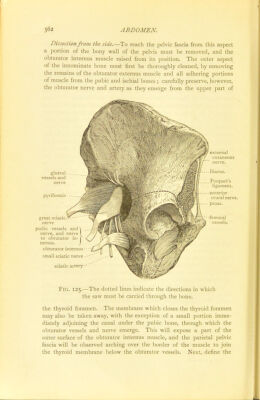
![the dissection must be made. Sejimgjhjrtjthj^_fo thej^chmijiej^ make the dissection on the rightside. ■I —, _ -ii. »_ i n~. I'M i. »« ~ .. ~ *■ ' - . — i — ,i ■ ■ Dissection from above.—This dissection is undertaken with the view of exposing the pelvic aspect of the fascia. Strip the peritoneum from the right side of the pelvic wall by means of the fingers. It should also be partially removed from the same side of the bladder. On care- fully scraping away the loose fatty extra-peritoneal tissue with the handle of the knife, or better still, with the finger nails, the pelvic fascia will be brought into view. To expose it in front, the bladder must be forcibly dragged backwards from the pubic bones, and the inter- vening areolar tissue taken away. Ai^hja^°iGL4]ie_J2£lyisJ^ noHDe^mcounJ^^ sc^jnjnxJLhgJowjj^ Here it is so thick that it is beyond injur}' so long as we work with the fingers, or the handle of the knife, but laterally it is thin, and great care must be taken. The extra- peritoneal tissue which surrounds the internal iliac vessels must also be removed, and the relation of their parietal branches to the fascia made out. Dissection from below.—The object of this dissection is to expose the perineal surface of the fascia. The pelvis must be placed so that the outlet looks upwards. The fat having previously been removed from the ischio-rectal fossa, divide the inferior hemorrhoidal vessels and nerves if they are still present, and then raise the levator ani muscle from the side of the rectum. To do this the muscle must be cut transversely about an inch above the anus. At^fb^tw_th^erotox^JlLKiil be_obsj^2{edJpj^ejU^ sejgaxsj[ejijjam_it) how^vgr, b^jt^kmarJiedJ^ but, as the dissector proceeds with the dissection, the muscle will be found higher up to be in close contact with the under surface of the visceral layer of the pelvic fascia. Lastly, he will come to the line of origin of the muscle from the pelvic fascia, i.e., the line along which the visceral layer leaves the parietal layer—and here he must stop. In the dissection of the ischio-rectal fossa (p. 353), the parietal pelvic fascia was exposed and recognised as forming the outer wall of the space. The entire inner surface of the parietal portion, both in its pelvic and perineal parts, is, therefore, now displayed, and, if the levator ani be drawn outwards and the pelvis held up to the light, the visceral pelvic fascia will be seen passing inwards from the parietal part of the aponeurosis to the viscera. But it is also necessary to obtain a view of the outer aspect of the parietal pelvic fascia, and, for this purpose, the following dissection must be made. VOL. I.—36](https://iiif.wellcomecollection.org/image/b21932979_0001_0593.jp2/full/800%2C/0/default.jpg)