Licence: Public Domain Mark
Credit: Indurative mediastino-pericarditis / by Thomas Harris. Source: Wellcome Collection.
20/78 page 14
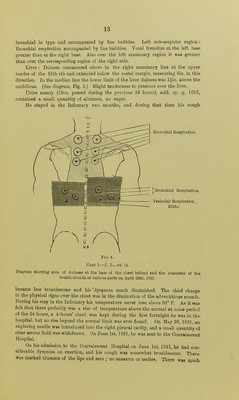
![enlargement of the liver, and some effusion in the right pleural cavity. The urine contained a small quantity of albumen. About a week after admission he became worse, he was troubled with sickness and took very ittle food. The cyanosis and dyspnoea became more marked, and the fluid in the right side of the chest increased in quantity. On July 14, 28oz. of pale, clear fluid were removed by means of an aspirator from the right pleural cavity. This appeared to relieve the dyspnoea for a time, and the cyanosis became less marked. On August 3rd, however, it was necessary to again puncture the right pleural cavity, and on this occasion 42^ oz, of clear fluid were removed. This was not followed by so much relief as the previous aspiration, and the boy gradually sank and died on August 12, 1891. During the last fortnight of life a considerable amount of anasarca of the lower extremities and ascites appeared. The amount of albumen in the urine increased. On August 10th, two days before death, it was noted that the urine was acid, sp. gr. 1018, contained about one- eighth albumen, was free from sugar, and no casts could be found. The post-mortem examination was conducted, on August 12th, in my ' presence, by Dr. J. E, Piatt, at that time the Resident Medical Officer to the Institution, who has kindly furnished the following report:— Adherent pericardium ; indurative mediastinitis with caseous affection in mediastinum. Thickened left pleura; effusion in right pleura; dilatation of heart; venous engorgement of liver and kidneys ; anasarca and ascites. Marked cutaneous hypostasis; considerable anasarca of the lower extremities, none of the uppei*. Left side of the chest slightly retracted; an old cicatrix of small size in the left lower axillary region. [This was the result of the operation of draining the left pleural cavity, performed twelve months previously at the Consumption Hospital.—T. H.] Rigor mortis was well marked in the lower extremities; less so in the upper. The abdomen contained a considerable quantity of clear, pale yellow fluid. There were no adhesions in the peritoneal cavity, and no signs of inflammation of the peritoneum. Pleurae: There was a large amount of clear pale yellow fluid in the right pleural cavity. The right lung was free from adhesions to the chest wall, except a few old adhesions over the apex. There were no adhesions of the right lung to the diaphragm, but old, tough, firm adhesions united its inner aspect to the mediastinum and to the external surface of the pericardium. The anterior edge of the right lung was about three-quarters of an inch to the right of the median line. The left pleural cavity was obliterated by firm, old, tough adhesions, the left lung being united to the chestwall, dia- phragm, and mediastinum. The parietal layer of the left pleura over the lower half of the chest was very much thickened ; in places it was half an inch in thickness. Pericardium : The cavity was obliterated by firm, old adhesions, which closely united the visceral with the parietal layer. Mediastinum: In the anterior and middle mediastinum, imme- diately above the heart, and extending from there to the upper part](https://iiif.wellcomecollection.org/image/b20421011_0020.jp2/full/800%2C/0/default.jpg)





 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image