Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine.
- Babcock, Robert H. (Robert Hall), 1851-1930
- Date:
- 1910
Licence: Public Domain Mark
Credit: Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
132/888 page 108
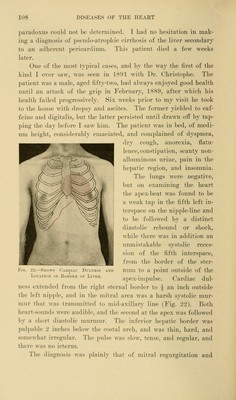
![paradoxus could not be detennined. I had no hesitation in mak- ing a diagnosis of pseudo-atrophic cirrhosis of the liver secondary to an adherent pericardium. This patient died a few weeks later. One of the most typical cases, and by the way the first of the kind I ever saw, was seen in 1801 with Dr. Christophe. The patient was a male, aged fifty-two, had always enjoyed good health until an attack of the grip in February, 1880, after Avhich his health failed progressively. Six weeks prior to my visit he took to the house with dropsy and ascites. The former yielded to caf- feine and digitalis, but the latter persisted until drawn off by tap- ping the day before I saw him. The patient was in bed, of medi- um height, considerably emaciated, and complained of dyspncea, dry cough, anorexia, flatu- lence, constipation, scanty non- albuminous urine, pain in the hepatic region, and insomnia. The lungs were negative, but on examining the heart the apex-beat was found to be a weak tap in the fifth left in- terspace on the nipple-line and to be followed by a distinct diastolic rebound or shock, while there was in addition an unmistakable systolic reces- sion of the fifth interspace, from the border of the ster- num to a point outside of the apex-impulse. Cardiac dul- ness extended from the right sternal border to ^ an inch outside the left nipple, and in the mitral area was a harsh systolic mur- mur that was transmitted to mid-axillary line (Fig. '22). Both heart-sounds were audible, and the socoiid at the apex was followed by a short diastolic murmur. The inferior hepatic border was palpable 2 inches below the costal arch, and was thin, hard, and somewhat irregular. The ])ulse was slow, tense, and regular, and there was no icterus. The diagnosis was jdainly that of mitral regurgitation and Location of Border of Liver.](https://iiif.wellcomecollection.org/image/b21229533_0132.jp2/full/800%2C/0/default.jpg)