Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine.
- Babcock, Robert H. (Robert Hall), 1851-1930
- Date:
- 1910
Licence: Public Domain Mark
Credit: Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
142/888 page 118
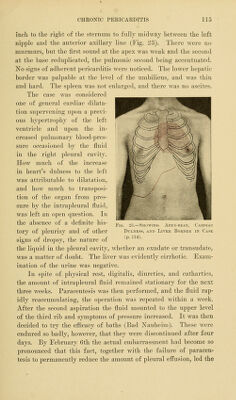
![larly frequent in cases of chronic mediastinopericarditis, and these may prove the cause of death. Physical Signs.—Inspection.—The ease and certainty with which adherent ])cricardiuni can be recognised clinically depend upon the situation and extent of the adhesions. If the sac is bound down to the heart, but not to surrounding parts, the condi- tion does not of a necessity produce recognisable physical signs, and this fact explains why sinechia pericardii is so often first de- tected on the post-mortem table. In the cases in which an adher- ent pericardium is diagnosed there are generally adhesions be- tween the sac and some of the surrounding structures, as the ante- rior thoracic wall, the pulmonary pleura on either side, and the diaphragm. Accordingly, it is in cases of chronic indurative mediastinoperi- carditis that the diagnosis is most easily and frequently made. This is owing to the fact that the existence of adhesions interferes witb the change in form and position of the heart normally occasioned by ventricular systole. During this phase in its contractions the heart becomes depressed at its base, and assuming a more rounded shape thrusts its point forward, upward, and towards the left, and thus produces the impulse against the chest-wall known as the apex-beat. It is evident that if adhesions restrict these movements the heart will of a necessity pull on the part to which it is bound. This pulling action is exerted during ventricular s3'stole, and con- sequently the most obvious and the most frequently observed sign of adherent pericardium is a I'isihlc systolic recession of the chest- wall. It may be perceived in various situations, but most com- monly in the neighbourhood of the apex-beat. Only a very lim- ited area may be thus drawn inward, but in most instances a systolic sinking takes i)lace in several of the interspaces near the apex and even in the e])igastrium, the extent and location of the adhesions determining tlie extent and position of this sign. It is best observed by placing the patient in a strong light, and then looking at the bared chest from above downward or from one side to the other. It is well to have the ])atient suspend respiration for a mo- ment wliilc inspection is being iiiadc, that tlie observer may not be deceived or confused by sinking of the soft parts incident to move-](https://iiif.wellcomecollection.org/image/b21229533_0142.jp2/full/800%2C/0/default.jpg)