Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine.
- Babcock, Robert H. (Robert Hall), 1851-1930
- Date:
- 1910
Licence: Public Domain Mark
Credit: Diseases of the heart and arterial system : Designed to be a practical presentation of the subject for the use of students and practitioners of medicine. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
80/888 page 56
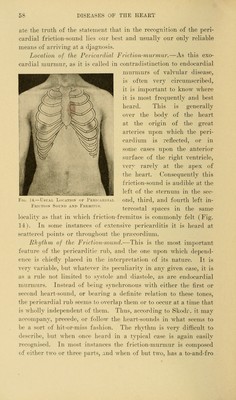
![dyspnopa is not likely to be marked iiulil the acute inflammatory process gives place to extensive etfusion. Respiration may be accelerated, but there is not actual air-hunger. In many instances, as previously stated, this affection remains so latent that if the physican were to rely for its detection upon subjective manifestations, the disease would surely be overlooked. For this reason the medical attendant should make daily examina- tions of the heart as a matter of routine practice, in all cases of rheunuitic fever or other infectious diseases capable of lighting uj) ])eri('ardial inflannnation. Course and Termination.—If an acute dry pericarditis is circumscribed, the plastic exudate not involving the whole sac, the activity of the process may speedily subside, and all evidence of its existence disappear in the course of a few days or a week. If, on the other hand, the inflammation is intense, and involves the myocardium, or if the plastic exudate is poured out over the entire organ, the course of the disease may extend over several weeks. In such cases, particularly in children with already existing valvu- lar disease, death is not unlikely, or if the patient recovers, he is likely to be left with a damaged heart. Acute cardiac dilatation is not infrequent, as shown by Poyn- ton's statistics. Indeed, all clinical observers of much experience with pericarditis in children have come to look upon dilatation of the heart as a quite general result, and to regard its occurrence with considerable apprehension. The extension of the inflamma- tion to the myocardium is a matter of grave danger, and one that is likely to result fatally. If flbrin be deposited in a thick layer over the entire surface of the dilated organ, it may act as a me- chanical hindrance to the subsequent return of the heart to normal size. This extensive fibrinous exudation results, furthermore, in an adherent pericardium, which will be described in a subsequent cha])ter. Physical Signs.—Tnspeciion.—From the very nature of acute fibrinous pericarditis it is evident that no information of more than a merely negative kind can be derived from an ocular examination of the patient. The countenance may express anxiety or suffering, and inspection of the chest may note some disturb- ance of respiration or an exaggerated and rapid heart-beat; but if there be evidence of deranged circulation this will probably](https://iiif.wellcomecollection.org/image/b21229533_0080.jp2/full/800%2C/0/default.jpg)