A manual of examination of the eyes / by E. Landolt ; translated by Swan M. Burnett ; revised and enlarged by the author.
- Landolt, E. (Edmond), 1846-1926.
- Date:
- 1879
Licence: Public Domain Mark
Credit: A manual of examination of the eyes / by E. Landolt ; translated by Swan M. Burnett ; revised and enlarged by the author. Source: Wellcome Collection.
339/340
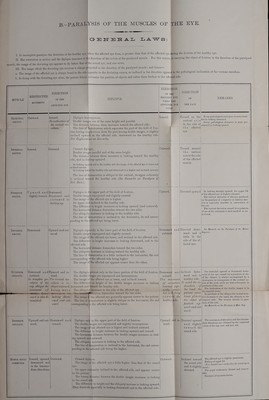
![i B.-PARALFSIS OF THE MUSCLES OF THE EYE. I I. In incomplete paralysis the deviation of the healthy eye, |vhon tlie affected eye fixes, is greater than that of the affected oye during the fixation of the healthy eye. ir. The restriction in motion and the diplopia increases in tlje direction of the action of the paralyzed mnscle. For this reason, in carrying the object of fixation in the direction of the paralyzed muscle, the image of the deviating eye appeal's to fly before that of ^e sound eye, and vice versa. 111. Tlie image whicli the deviating eye receives is always pjojected in the direction of the paralyzed muscle; and hence— a. The image of the affected eye is always found to the side jipposite to the deviating cornea, or inclined in the direction oppose! to the pathological inclination of the vertical meridian. b. In fixing with the deviating eye alone, the patient falsely pstimat^ the position of objects and refere them farther to the affected side. MUSCLE EESTRICTED MOVEMENT. DIRECTION OF THE AFFECTED EYE DIPLOPIA EXTEllNAL BECTUS. Internal RECTUS. Inward. Superior RECTOS. Inferior RECTOS. Outward. Inward. No inclination of j the vertical vie- 1 ridian. Dijiiopia homonymous. Double images are of the same height and parallel. Tlie distance between them increases toward the affected side. The line of demarcation which separates the pavt of the field of fixa- tion having single visioii from the part having double images, is slightly nclined upward on the affected side, downward on the healthy side. For Explanation see Remarks. Outward. Crossed diplopia. Outward; Double images parallel and of the same height. The distance between them increases in looking toward the healthy side, and in looking upward. Ill louking ii|nviird nml lo tlic heiiUliy side llie imnge of llie iifiected eye is lower niid tiiclhicd iiiwnrd. In looking lowiird the iiealthy aide and downward it is higher and ineliiied outwurd. The line of demarcation is obHque to the vertical, its upper extremity inclined toward the healthy side {See Bemarks on Faralysis of Ext. Beet.) Upward an dlDownward. ilightly inward. Dowmoard and outward looHng up. Upward and out- ward. SUI'EIIIOR OBLIQDE. Diplopia in the upper part of the field of fixation. Double images superposed and slightly crossed. The image of the affected eye is higher. It.s upper end inclined to the healthy side. The difi'erence in height increases in looking upward {and outward). The horizontal distance diminishes toward the two sides. The obliquity increases in looking to the healthy side. The line of demarcation is inclined to the horizontal, its end corres- ponding to the affected eye being lower. DIREO^^ON OF THE HEALTHY EYE WHEN THE AFFECTED EYE FIXES 1 DIRECTIOIT REMARKS Inward. I Turned o vertical Upward. Dii)lopia especially in the lower part of the field of fixation. Double images superposed and slightly crossed. The imnge of the affected eye lower, and inclined to the affected side The difference in height increases in looking downward, and to the ffected side. The horizontal distance diminishes toward the two sides. The obliquity increases in looking toward the healthy side. The line of demarcation is a little inclined to the horizontal, the end corresponding to the affected side being higher. The image of the affected eye appears nearer than the other. Downwan: outwan., iDownward and Upward and I outward. ward. complete pa-, The vertical vie- j ralysia of (Aej vidian is sup. oblique the dined outward,\( movement of'i being more ' 'rtAflf^rt/Tl^ ^ffevflWl*!•f^i^Hfli^B^ ■'V ward is also di-j looking dovm- minished. ward and out- ward. Inferior OBLIQUE. Upward and out- ward. Downward and inward. Motor oculi communis. Inward, upward, downward and in the interme- diate directions. The diplopia present only in the lower portion of the field of fixation. The double images are saperposfd and homonymous. The image of the affected eye is lower, and inclined inward. The difference in height of the double images increases in looking lownwjud and toward the healthy aide. Tlie ob]i<|uity increases to the side of the affected eye. '^'ftu ^iimi'ul ^^ration diminishes toward the two sides. The image c' tho affected eye generally appeara nearer to the patient, The line of emarcation is slightly oblique to the horizontal, the end corresponding o the affected side being lower Downwarq and inward, mo ■cment Turned around the vertical axis to the side of the affected muscle. Directed upward and 1 the' Every palliological i;(mivrgenc<- is more mani- ^ J g fest in lookinij; liowniaivd. ' Every pjithologieal diveri/encc is more pro- to the Side ot ^^y^j.^,, ij^gj-jug the' affected j eye. Directed down^ ward and i little to the side of the af- fected eye. Diplopia onl; in the upper part of the field of fixation. The double i nages are superposed and slightly homonymous. Upward aiid in- ward. Outward. Tlic iniiige o: The differenc the affected eye is higher and inclined outward, height increases in looking upward and inward. The horizont .1 distance between the double images increases in look' ing upward anc outward. The obliquitj increases in looking to the affected side. The line of d marcation is inclined to the horizontal, the end corres ponding to the ffected side being the higher. Crossed diplobia. The image of the affected eye a little higher than that of the sound eye. Its upper exti emity inclined to the affected side, and appears nearer to the patient. Tlie lateral diitance between the double images increases in looking to the sound aidi-. The differenct in height and the obliquity increase in looking upward. They diminish eipecially in looking downward and to the affected aide. Outward. In looking strongly upward, the upper Hd of the fifiected eye is slightly elevated. Tlie vertical deviation of the eye, produced by the paralysis of a superior oi' inferior rec- tus 13 especially manifest in abduction of the eye. The vertical deviation caused by a piiralysis of one of tlie obliqdes is most marked in ad- duction. See Reimrh on the Paralysis of the Rectus Sup,rior. Inclined down ward and to healthy side. To avoid the in- clination of tlie head, the patient some- times places the object of fixation up- ward and out- ward. The restricted upward or downward move- ment of the eye, caused by a paralysis of one of the obliques, is ohvaya accompanied by a convergence, in consequence of the isolated ac- tion of the recti, while we find a dirertjence in panilyBis of the recti. The inclination of tlie double images is in the opposite aeiisc. In paralysis of the obUqufg the vertieal devta- lioii increases lo tlie nasal, the ohliquitij to the temporal side. The reverse obtains in para- lysis of the rtcH. Sm Remarks on the ParahjBia of Bed. Sup. Directed upward and slightly toward the sound side. The maximum of elevation and tlie interme- diate directions are obtained by the combiued action of the sup. rect. and rect. ext. Inclined toward the sound side and is slightly elevated. The affected eye is slightly proniinent. Falling of upper lid. {It i.'> elnyjtetl more easihi u-hen the sound eye M The pupil moderately dilated and immov- able. Paralysis of accommodaiion.](https://iiif.wellcomecollection.org/image/b20393167_0339.jp2/full/800%2C/0/default.jpg)