[Report 1932] / School Medical Officer, Somerset County Council.
- Somerset Council
- Date:
- 1932
Licence: Attribution 4.0 International (CC BY 4.0)
Credit: [Report 1932] / School Medical Officer, Somerset County Council. Source: Wellcome Collection.
19/52 (page 17)
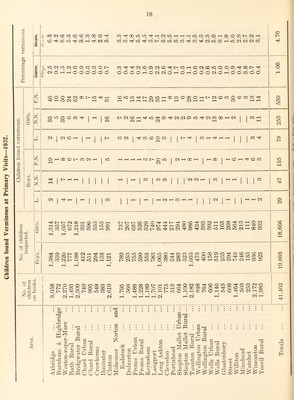
![While the work clone is most valuable and the “value tor money’’ is definitely high there are certain unsutisiactory features about tlie dental work. In the first place, tliree dentists cannot keep pace with the work. Each child in the scheme should be seen again after approximately a year, and it will he agreed that this is rather a long interval and should not be exceeded. Instead, their examination tends to fall later, so that the child may not be re-examined for to 1| years. The yearly total time of delay each year is about 126 days, while at the end of the year (11)152) it was about 4113 days, or ecjual to the time of 1.9 dentists. Only a small portion of this is accounted for by illness of one or more dentists. There is evidence, as I pointed out in my report for last year, that the amount of dental decav of the children entering the scheme is increasing and that the teeth of school entrants are worse than they were in the earlier days of the scheme. It would be a great advantage to let the children into the scheme at 5 and 6 instead of as at present 6 and 7 years of age, but that cannot be undertaken with the present staff. There is a close relationshij) between dental decay and nutrition, and there is much need for improving the feeding and nutrition standards of the pre-school child. The figures given on page 16 of the ages of the children examined do not show that progressive increase which they should do. This means that many children drop out of the scheme when older. Part of this is due to transference to secondary schools, there being no dental treatment given for these children, but this can only account for a small part. The change froui a Junior to a Senior school often makes a break, and in the new' school the children may not be in¬ cluded in the scheme, but we try to counteract this by notification to the Head Teacher of all the children who were in the scheme. Evidently less attention is paid by the parents to the teeth of the older children and many are allow'ed to dro]) out of the scheme. The lag in treatment is purely a question of staff; starting the scheme at 5 years is also a Staff matter. Steps could be taken to put more pressure upon ]);irents in the scheme who now let their children leave it, and this would result in better figures. To do this would, however, still further weigh the scheme and add more children to be examined when we are already behind. These defects of the scheme cannot be dealt with effectively until the present dental staff is increased. VERMINOUS CONDITION OF SCHOOL CHILDREN. This condition has so improved of recent years that it has not been necessary to make complete inspections of every child in every school, but the best results have been obtained by concentration upon schools and individual children needing attention. It has not been possible, therefore, accurately to compare conditions now with what existed many years ago. To enable this to be done, a complete examination of all the children was made dui'ing 1932, every school being visited and every child in attendance examined. These visits were of course paid without notice being given, and followed the same procedure as in earlier years. If anv- thing the criteria woidd be more stringent, the imja-oved conditions allowing a higher standard. The data, therefore,, is strictly comparable with the findings in earlier years. The results obtained are shown in the Table,](https://iiif.wellcomecollection.org/image/b30112266_0021.jp2/full/800%2C/0/default.jpg)