'Cremotres' triple sulfonamide suspension : a triple sulfonamide combination that reduces renal crystalluria / Sharp & Dohme.
- Merck & Co.
- Date:
- 1949
Licence: Public Domain Mark
Credit: 'Cremotres' triple sulfonamide suspension : a triple sulfonamide combination that reduces renal crystalluria / Sharp & Dohme. Source: Wellcome Collection.
3/4
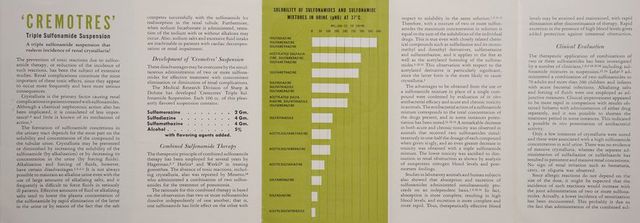
![fonamides can be discontinued as a rule before the time when allergic reactions appear most frequently.!2 A triple sulfonamide combination has been em- ployed in treating several hundreds of patients with acute pneumonia with excellent therapeutic results and no evidence of renal concretions. Similar good results have been obtained in gon- orrhea.14.15 On the basis of the above mentioned studies,!?.14 it would appear that the possibility of crystalluria is eliminated almost entirely with the use of a triple sulfonamide combination. This remarkable reduc- tion in the incidence of crystalluria is advantageous when it is desirable to administer a larger than ordinary dosage for treatment of resistant infec- tions, since the danger of crystalluria is not there- by increased. Sulfamethazine rather than sulfathiazole has been included in ‘Cremotres’ because of the rela- tively high incidence of toxic reactions following sulfathiazole therapy (18 per cent), and in accord- ance with the proposed deletion of this compound from New and Nonofficial Remedies.!* Numerous reports have appeared in the medical literature with respect to the clinical efficacy and lack of toxicity of sulfamethazine (4,6-dimethy]l- 2-sulfanilamidopyrimidine). With respect to acute and chronic toxicity, this compound appears to be similar to sulfamerazine and sulfadiazine.?° On the basis of solubility and renal toxicity, however, sulfamethazine and sulfamerazine may be more desirable drugs than sulfadiazine. ‘‘Sulfamethazine seems to be devoid of renal toxicity, irrespective of the concentration of this drug in the blood. Sulfamerazine has decidedly less renal toxicity than sulfadiazine,’ the most important factor apparently being the greater solubility of sulfamethazine and sulfamerazine in acid urine.2° In formulating a triple sulfonamide preparation suchas ‘Cremotres’, there- fore, the addition of sulfamethazine should be of definite value in preventing renal toxicity and en- hancing the therapeutic efficacy of the combination. Clinical Indications ‘Cremotres’ is recommended for the treatment or infections in which sulfamerazine,2!-25 sulfadia- zine,2630 or sulfamethazine,*!%5 alone is indicated. This triple sulfonamide preparation is a pleasantly flavored suspension, especially suitable for infants and small children in whom the administration of sulfonamides in tablet form frequently presents a problem. Dosage Adults: Initial dose 2 tablespoonfuls (3 Gm. of sulfon- amide) followed by 2 teaspoonfuls (1 Gm.) every 4 hours. Children: Up to 6 months—Initial dose 1% teaspoonfuls (0.75 Gm.) followed by % teaspoonful (0.25 Gm.) every 6 hours. Y% to 3 years—Initial dose 3 teaspoonfuls (1.5 Gm.) followed by 1 teaspoonful (0.5 Gm.) every 6 hours. 3 to 10 years—Initial dose 2 tablespoonfuls (3 Gm.) followed by 2 teaspoonfuls (1 Gm.) every 6 hours. Note: In the above dosage schedules 1 teaspoon- ful is assumed to be equivalent to 5 cc. and 1 tablespoonful to 15 cc. Attention is called to the potential error in the use of household units: A teaspoonful may hold from 4 to 7 cc. and a table- spoonful may hold from 15 to 22 cc. It is recom- mended, therefore, that a medicinal spoon or cali- brated medicine glass be used to dispense the individual doses suggested above. The maintenance dosage of ‘Cremotres’ should be continued until definite clinical improvement has been obtained, as indicated by defervescence. The recommended dosage may be adjusted de- pending upon the nature of the illness and the condition of the patient, in accordance with clin- ical judgment. Although it is anticipated that the joint use of the three sulfonamides in ‘Cremotres’ will reduce the occurrence of crystalluria to a minimum, the added protection of alkalizing salts and fluids is nevertheless recommended when practical, espe- cially in older patients and in those receiving high dosages for prolonged periods. The precautions usually employed in sulfonamide therapy should be observed. The total sulfonamide concentration in blood and urine may be determined by standard procedures, as described in an informative brochure that is available on request. How Supplied ‘Cremotres’ Triple Sulfonamide Suspension is sudaes in ‘Spasaver’ bottles containing 16 fluid- WONIMLNNO MA 22502623765 Sharp & Dohme PHARMACEUTICALS - BIOLOGICALS Philadelphia 7, Pa. WELLCOME LIBRARY References 1. Lehr, D., J. Urol. 55:548, May 1946. 2. Lehr, D., Slobody, L., and Greenberg, W., J. Pediat. 29:275, Sept. 1946. 3. Flippin, H. F., and Reinhold, J. G., Ann. Int. Med. 25:433, Sept. 1946. 4. Editorial, New England J. Med. 236:842, May 29, 1947. 5. Snyder, L. J., Proc. Central Soc. Clin. Research 20:70 (1947). 6. Hagerman, G., Nordiskt med. Ark. 22/1093, 1223 (1944). 7. Hagerman, G., Nordiskt med. Ark. 24:1944 (1944). 8. Herlitz, S., Nordiskt med. Ark. 22/1226 (1944). 9. Werk6, L., Svenska Lakartidn. 42:746 (1945). 10. Mineo. L. P., New York State J. Med. 44:2022, Sept. 15, 1944. 11. Lehr, D., Proc. Soc. Exper. Biol. & Med. 58:11, Jan. 1945. 12. Lehr, D., Proc. Soc. Exper. Biol. & Med. 64:393, April 1947. 13. Lehr, D., Brit. M. J. 2:943, Dec. 13, 1947. 14. Frisk, A. R., Hagerman, G., Helander, S., and Sjégren, B., Brit. M. J. 1:7, Jan. 4, 1947. 15. Nilzen, A., Svenska Lakartidn. 43/1816 (1946). 16. Lehr, D., Brit. M. J. 2:543, Sept. 18, 1948. 17. Oettinger, L., Jr., and Cronheim, G., Am. Practitioner 2:526, April 1948. 18. Ledbetter, J. H., and Cronheim, G. E., Am. J. M. Sc. 216/27. July 1948. 19. Report of Council on Pharmacy and Chemistry, J.A.M.A. 136:691, March 6, 1948. 20. Schmidt, L. H., Hughes, H. B.,and Badger, E. A.,J. Pharmacol. & Exper. Therap. 81:17, May 1944. 21. Flippin, H. F., Gefter, W. I., Domm, A. H., and Clark, J. H.., Am. J. M. Sc. 206:216, Aug. 1943. 22. Anderson, D. G., Oliver, C. S., and Keefer, C. S., New England J. Med. 230:369, ”March’ 30, 1944, 23. Genecin, A., Austrian, R. C., and Nelson, R. A., Bull. Johns Hopkins Hosp. 765112; March 1945. 24. Reinhold, J. G., Flippin, H. F., Zimmerman, J. J., Gefter, W. I., and Riddler, J. G., J. Clin. Investigation 24:352, May 1945. 25. Forbes, G. B., Perley, A., and Dehlinger, J., J. Pediat. 28:24, Jan. 1946. 26. Finland, M., Strauss, E., and Peterson, O. L., J.A.M.A. 116:2641, June 14, 1941. 27. Finland, M., Peterson, O. L., and Goodwin, R. A., Jr., Ann. Int. Med. 17:920, Dec. 1942. 28. Shackman, N. H., and Bullowa, J. G. M., Arch. Int. Med. 72:329, Sept. 1943. 29. Marangoni, B. A., and D’Agati, V. C., Am. J. M. Sc., 207:67 Jan. 1944. 30. Appelbaum, E., Am. J. M. Sc. 207:492, April 1944. 31. Loughlin, E. H., Bennett, R. H., and Flanagan, M. E., J. Lab. & Clin. Med. 29:568, June 1944. 32. Volini, I. F., Engbring, G. M., and Schorsch, H. A., Arch. Int. Med. 75:168, March 1945. 33. es T. N., and Wylie-Smith, R., Lancet 2:731, Dec. 11, 34. Melton, G., Lancet 1:277, Feb. 26, 1944. 35. Ramsay, W. A., Luxton, R. W., Steiner, P., and Smith, G. S., Lancet 1:78, Jan. 20, 1945. A-1145 150M 1049 PRINTED IN U.S.A.](https://iiif.wellcomecollection.org/image/b3347316x_0003.jp2/full/800%2C/0/default.jpg)