Diseases of the larynx / by Dr. J. Gottstein ... trans. and added to by P. M'Bride.
- Jacob Gottstein
- Date:
- [1883]
Licence: Public Domain Mark
Credit: Diseases of the larynx / by Dr. J. Gottstein ... trans. and added to by P. M'Bride. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
113/290 (page 101)
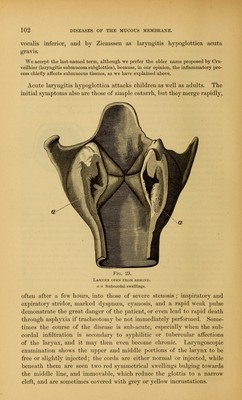
![impanied by tuberculosis, offered in other respects the characteristic appearances of laryngitis hypoglottica, C. E.. aged thirty-three, consulted us in the summer of 1882 on account of cough and hoarseness.—Infiltration of both apices and tubercular ulcer in the interarytenoid com- re. Treatment—Narcotics, milk, local application of carbolic acid (1-100 of glycerine . The patient so far improved that he was able to resume his work, but in October he returned considerably worse, and suffering from breathlessness and suffocation at night. Laryngo- scopy examination gave the following results : Mucous membrane of the upper and middle portion of the larynx injected but not swollen, ulceration of the interarytenoid fold, vocal cords reddened, and underneath them two red tumours almost touching in the middle line, which did not separate even on deep inspiration i Fig. 22 . Respiration could only occur through a narrow opening which remained between the vocal procenocn, and the patient was adv. to go into hospital in order to have tracheotomy \ ^i - formed. He was admitted on the 17th, and everything was ready for the operation, which was only delayed because the patient felt fairly well when at rest. On the morning of the 20th he was found in bed threatened with asphyxia, and, while tracheotomy instruments were being brought.insensibility occurred. There was marked cyanosis, respiration at intervals of fifteen seconds. and a rapid weak pulse. Tracheotomy was performed a> quickly as possible, and a small quantity of blood flowed 00 into the trachea, respiration became better, the pulse improved, but there was no return of consciousness, the c *«J2gX*J b££££o£ patient dying forty-eight hours after the operation, observed by the Author. A complete aoto] sy was not allowed and only the larynx wai examined, with the following residt : Epiglottis, vestibide. and false cords reddened: apices of the arytenoids slightly (edematous : from the lower margins of the cords arise two symmetrical tumours, which become less marked, and finally lose themselves towards th,e trachea, the most marked swelling being immediately beneath the vocal cords (Fig. . Microscopic examination reveals subepithelial tubercular infiltration, together with numerous small round cells. In the vocal cords themselves there are no tubercular nodules, but only round cells, and the same applies to the subglottic swellings. In the latter the infiltration extends into the lax submucous tissue, although the cells ai numerous here than in the subepithelial layer. The infiltration is most marked in the glandules, but the individual acini are only here and there separated from one another by round cells, maintaining everywhere their normal shape, and thus affording evidence that the infiltration is recent. Around divided blood vessels are seen leucocytes, while muscles, perichondrium, and cartilage are normal. SYMPTOMS.—Acute diffuse submucous laryngitis begins with the symptoms of severe catarrh—hoarseness, croupy cough, and striduloua respiratioo ; the latter becomes more and more difficult, and assumes the character of Laryngeal stenosis. The symptoms of obstructed respiration when <»nly the upper or middle portions of the larynx are affected, how- ever, rarely assume such grave proportions as those of oedema glottidis, afterwards to be described. The severity of the symptoms is much -rearer in those cases in which the lower part of the larynx is involved, described by old authors 8 stier, Cruveilhier) as oedeme sousglottique, laryngite sousmuqueuse iglottique, and described more recently by Burow as chorditis](https://iiif.wellcomecollection.org/image/b21022641_0113.jp2/full/800%2C/0/default.jpg)