Licence: Public Domain Mark
Credit: Hand-book of surgical operations / by Stephen Smith. Source: Wellcome Collection.
Provider: This material has been provided by the National Library of Medicine (U.S.), through the Medical Heritage Library. The original may be consulted at the National Library of Medicine (U.S.)
60/280
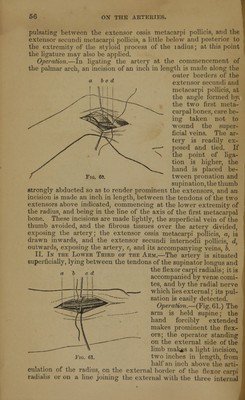
![a be def Fig. 6a II. In tiie Middle of TnE Arm.—The brachial descends on th« inner- side, first of the coraco-brachialis, and afterwards of tin biceps; it is covered by the fascia and in- teguments, and over- lapped slightly by the biceps; its sheath contains tlie- two venae comitea; the internal cutane- ous nerve lies supe^ ficial to it; the me- dian is superficial to it above, and rather to its outer side; about the middle of the arm, it crosses the artery, and in- teriorly it is to its ulnar side ; the ulnar nerve is internal to the artery, and at some distance from it inte- riorly ; the spiral nerve is posterior, and separates it above from the triceps. Operation.—(Fig. 64.) The arm is extended and carried at right angles to the body, and held supine. The course of the artery may be recognised, 1. By its pulsation; 2. By the internal margin of the biceps and coraco-brachialis; 3. By the median nerve, to the inner side of which it lies; 4. By the line above given. An incision is made two or three inches in length, along the inner border of the (1 e biceps, dividing the skin freely down to the fasciae; this is in- cised on a director, and the position of the median nerve detected in the wound with the finger; this is exposed, and being pushed asidt with the biceps, d, and the median nerve, b, the artery, c, is found im- mediately behind anc inside, accompanied b] its venae comites, a The arm is now flexec the vessel isolated, and the ligature passed from without inwards. Modifications.—If the incision is made a little too far back the ulna nerve is exposed, and is liable to be mistaken for the median; an](https://iiif.wellcomecollection.org/image/b21155458_0060.jp2/full/800%2C/0/default.jpg)