Volume 1
The regulation of private and other independent healthcare : fifth report / Health Committee.
- Great Britain. Parliament. House of Commons. Health Committee
- Date:
- 1999
Licence: Open Government Licence
Credit: The regulation of private and other independent healthcare : fifth report / Health Committee. Source: Wellcome Collection.
46/68 page 44
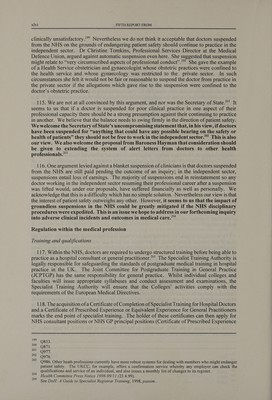
![106. Those figures suggest that each region would have a sufficient number of establishments to inspect to make a regionally-located inspectorate perfectly viable. We do not believe this situation would be very much altered under the new regional structure. The licensing process 107. The current sanctions available to registration and inspection units have been criticized for their lack of range. Units can cancel the registration of an existing facility, or refuse to register a new one, or issue warnings. The Secretary of State described this choice as being “between a nuclear weapon and a feather duster”.'*° We agree with the Secretary of State that a wider range of powers for the regulatory authorities than are presently available would be appropriate. We think, for example, the regulator should be able to license a home or clinic to carry out certain activities but not others. A possible model might be the Human Fertilisation and Embryology Authority (HFEA), which has powers to grant licences with or without conditions, suspend them or revoke them. In granting licences it requires certain general conditions to be complied with while additional conditions may be added specifically relevant to the centre concerned.'*’ 108. We also favour the approach the HFEA takes towards establishing line-management responsibility for the activities of the clinics it deals with. It is the duty of the individual named as the Person Responsible for each centre to ensure that licence conditions are complied with. To assist them, the HFEA is required by law to produce a Code of Practice to guide clinics on how they should carry out their licenced activities.'** The advantage of this approach, in our view, is that it helps shift the burden of establishing compliance from the regulatory authority to the service provider. We recommend that the Secretary of State creates a licensing regime for the independent acute sector offering a wide range of powers and sanctions which places the burden of proof of compliance on the provider, not the regulator. We would like the Independent Regulator to issue a detailed code of practice with a view to ensuring that consistent national standards of inspection apply to the independent healthcare sector. 109. Going beyond formal regulatory structures, we note the view of the RCN that it is important that regulation provides more than a policing function “to include a facilitative, supportive and advisory role too, i.e. not just identifying what the weaknesses/ failures are, but also looking at why they are occurring, and advising on how improvements can be made”.'® One of the criticisms that the Institute of Chartered Secretaries and Administrators made of the current system was that reports “fail to praise good practice or give positive encouragement to staff’.'° It is our view that a good regulatory regime will actively raise standards rather than merely check existing rules are complied with. Suspended clinicians 110. The Department informed us that the Government was aware of concerns about the relationship between the NHS and the private sector in disciplinary cases “and particularly that doctors who have been suspended from work by their NHS employer may continue to work in the private sector”.'*' In oral evidence, the Secretary of State drew attention to the Rodney Ledward case, pointing out: “It was not very long ago that we had an obstetrician and gynaecologist in Kent who had, quite rightly, been suspended from work in the National Health Service because he was injuring large numbers of female patients but who was still literally operating on private patients in private hospitals”.'” 186 187 188 189 190 19] Q909. Ev., p446. Ibid. Ev., p308. BV:, Hace: Ev., p4. % Q908.](https://iiif.wellcomecollection.org/image/b3222087x_0001_0046.jp2/full/800%2C/0/default.jpg)





 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image