The surgical treatment of the diseases of infancy and childhood / by T. Holmes.
- Timothy Holmes
- Date:
- 1868
Licence: Public Domain Mark
Credit: The surgical treatment of the diseases of infancy and childhood / by T. Holmes. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
632/682
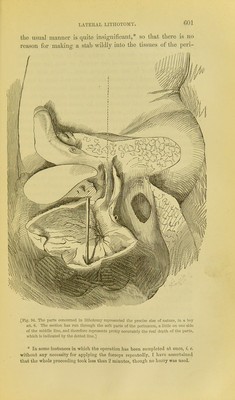
![nseum, instead of cutting through them in an orderly manner, and feeling from time to time for the staff. For this purpose the left forefinger should be used; and it also directs the knife towards the centre of the wound, so that the anterior part of the latter is not made too deep. Were this done, the urethra would be opened further forward than is neces- sary, and therefore the womid in it would be somewhat too large; the knife also would have to travel along the curved part of the staff, and there might be some additional trouble in reaching the bladder, and some additional risk of sKpping from the groove. The bulb also and its artery would probably be wounded; though this is not a matter of the same import- ance in children as in adults. When the groove is distinctly felt, the finger-nail should be ]Dlaced upon it, the point of the knife inserted, and then' passed along it into the bladder. If the incision has been made as above described, the slightly higher position of the bladder in early age as compared to its situation in the adult wiU be scarcely perceived in passing the knife into it. A sensation which I can hardly describe assiires the surgeon generally when the bladder is reached. It is due no doubt to the cessation of any resistance to the passage of the knife through the tissues. The knife can hardly be pushed too far, so as to wound the back of the bladder, if it be kept in the groove of the staff, for the latter terminates in a stop which would catch the point. Otlier- wise that accident might well occur, and it has occui*red, no doubt from the operator having quitted the groove. In with- drawing the knife, it is well to lateralise its edge, and thus slightly enlarge the incision. The left forefinger is now pushed along the groove of the staff until the opening has been so far enlarged that the finger can be got between the upper edge of the staff and the pubes, when it will readily enter the bladder. When it has done so, and when the stone is distinctly felt to be in contact with the finger (and not before) the staff is to be removed, the finger tiu*ned with its pulp upwards, and the forceps passed along the upper siu-face of the finger slowly into the bladder. There is often a little difficulty in children in seizing the stone, in consequence of its small size, smooth surface, and the way in which the walls of the bladder (often much enlarged) fall down over it.](https://iiif.wellcomecollection.org/image/b21511469_0632.jp2/full/800%2C/0/default.jpg)