On the theory and practice of midwifery / By Fleetwood Churchill. With notes and additions by D. Francis Condie.
- Fleetwood Churchill
- Date:
- 1859 [©1851]
Licence: Public Domain Mark
Credit: On the theory and practice of midwifery / By Fleetwood Churchill. With notes and additions by D. Francis Condie. Source: Wellcome Collection.
Provider: This material has been provided by the Harvey Cushing/John Hay Whitney Medical Library at Yale University, through the Medical Heritage Library. The original may be consulted at the Harvey Cushing/John Hay Whitney Medical Library at Yale University.
438/536 page 448
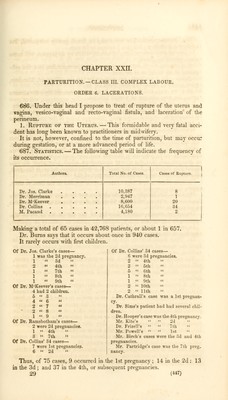
![6SS. Causes.—Various causes may give rise to it, and it may happen at different periods— 1. During gestation. — The form of extra-uterine pregnancy which is called interstitial filiation (§ 250) may give rise to it. The ovum, in- stead of passing direct from the fallopian tube into the uterine cavity, is retained in an interstice of the uterine fibres, where it grows, up to a cer- tain point. As it increases, the outer portion of the uterine parietes be- comes gradually thinner by absorption (as in the case of abscess), and at length gives way, and the feus is precipitated into the abdomen, con- verting the case into one of ventral fcetation. It may also be the consequence of disease, as in Mr. Else's and Dr. Spark's cases: from softening, and from abscess in the walls, as related by Duparcque. Any violent accident, such as a fall or a blow, may give rise to it. It sometimes occurs without any assignable cause ; the patient, perhaps, is awakened from sleep by it. It has been attributed to irregular action of the uterine fibres. 689. 2. During labour. — a. If the uterus have been attacked by in- flammation during pregnancy, its tissue may have been so much weakened or disorganized, that the violent contractions which take place during labour may rupture it, from the want of consentaneous action in the part affected, or from the pressure of some part of the child against it. Steidele relates a case where rupture occurred in consequence of gan- grene. My friend, Dr. Murphy, has published an excellent paper illustrative of this cause of rupture, with cases where the uterus was atrophied, thinned, or softened in texture. Duparcque quotes cases of thinning of the uterine walls, softening, scirrhus, and gangrene. In some cases, the seat of the laceration corresponds exactly with the situation of the previous pain. Dr. Tyler Smith believes that in many cases violent uterine action is in itself the cause of rupture ; the immediate cause being either emotion or volition, or a reflex, or peristaltic action. The period of labour at which the rupture may occur from this cause, will vary ; it may be at the beginning, before the rupture of the mem- branes ; during the passage of the head through the pelvis; or after the delivery. ;>. A certain amount of narrowing of the upper outlet may give rise to if. This is a purely mechanical cause. The head of the child is forced downwards by violent labour pains, but is unable to enter the pelvis, from the contraction of the upper strait; now if the pains continue with great ]tower, the head is turned to one side or the other, or posteriorly, and the only obstacle here being the uterine or vaginal parietes, the head is driven through them at the weakest part. They offer the less resistance, proba- bly, from the woman having generally borne several children. In one of Dr. Clarke's cases, the antero-posterior diameter of the upper outlet measured but 3 inches; in two others, 3^. In case 18 of Dr. Douglas, the pelvis measured but two inches antero- posterior^- ; and in another case (20) there was a bony ridge on the top of the symphysis pubis, to which the 'cut corresponded.](https://iiif.wellcomecollection.org/image/b2103011x_0438.jp2/full/800%2C/0/default.jpg)