A dictionary of practical surgery : comprehending all the most interesting improvements ... an account of the instruments ... the etymology and signification of the principal terms ... / by Samuel Cooper ; with numerous notes and additions ... together with a supplementary index ... by David Meredith Reese.
- Samuel Cooper
- Date:
- 1844
Licence: Public Domain Mark
Credit: A dictionary of practical surgery : comprehending all the most interesting improvements ... an account of the instruments ... the etymology and signification of the principal terms ... / by Samuel Cooper ; with numerous notes and additions ... together with a supplementary index ... by David Meredith Reese. Source: Wellcome Collection.
Provider: This material has been provided by the Woodruff Health Sciences Center Library at Emory University, through the Medical Heritage Library. The original may be consulted at the Woodruff Health Sciences Center Library, Emory University.
99/1188
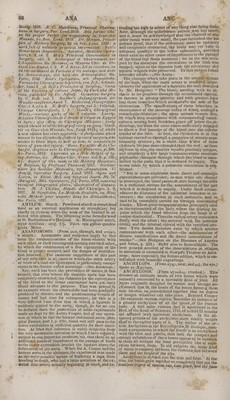
![le presorved for covering the end of the bone. On taking away a finger from a metacarpal bone, Mr. Sharp recommends making two small longitudinal inci- sions on each side of the joint, as a means of facilitating the separation. In amputating the fingers and toos, the operation is greatly facilitated by cutting into the joint when it is bent. Having made an opening in the back part of the capsule, one of the lateral ligaments may easily be cut, after whicli nothing keeps the head of the bone from being turned out, and the surgeon has only to cut through the rest of the exposed ligamentous and tendi- nous parts. Some recommend making a small Semicircular flap of skin to cover the bone ; but this is quite unneces- sary if care be taken toAlraw the skin a little up, and to cut where. Mr. Sharp directs. However, as making a small flap gives little pain, I have generally followed this method, though it appears to me nearly a matter of indifference which plan, is adopted. In operating at the joints between the phalanges and metacarpal bones, a flap should always be made, either ,o;i ■ the upper or under part of the fingers to be removed. > ! Although it is generally best to remove the fingers at the joints, it is sometimes thought right, where the injury just includes the joint and no more, to saw through the bone, instead of operating at the next ar- ticulation.—(See Guthrie on Gun-shot Wounds, p. 334.) The division can also be readily made with cutting plyers. It may happen, that the bones of the toes and only part of the metatarsal bones are carious, in which case the leg need not he cut off, but only so much of the foot as is disordered. A small spring saw is here the most convenient. When this operation is per- formed, the heel and the remainder of thevfoot will be of great service, and the wound heal up safely, of which Mr. S. Sharp says, he had in his time seen one example.—(Op. of Surgery, chap. 37, ed. 3.) Mr. Hey confirms this statement of Sharp's concerning the impropriety of removing the whole foot, when the me- tatarsarbones are carious, and every other part of the leg is sound, as the remainder of the foot is of im- mense service in walking, the use of the ankle not being destroyed. Mr. Hey describes a new mode of removing the me- tatarsal bones, which on repeated trial has fully an- swered his expectations. By the term new, I here mean a particular method, which had not been pre- viously described, though it may have been performed by others sooner th.ah by Mr. Hey himself; for the merit of having first done it is imputed to the late Mr. Turner, of North Yarmouth, who did it with success about the year 1787.—(See Hutchison's Pract. Obs. p. 70.) Mr. Hey makes a mark across the upper part of the foot, to denote where the metatarsal bones are joined to those of the tarsus. About half an inch from this mark, nearer the toes, he makes a trans- verse incision through the integuments and muscles, covering the metatarsal bones. From each extremity of this cut, he makes an incision along the inner and outer side of the foot to the toes; he removes all the toes from the metatarsal bones, and' then separates the integuments and muscles, forming the sole of the foot, from the inferior part of the metatarsal bones, keeping the edge of the knife arvnearthe bones as possible, in order to expedite the operation, and preserve as much muscular flesh in the .flap -as can be saved. He then separates tlie four smaller • metatarsal bones at their junction with the tarsus, and divides, with a saw, the projecting part of the first cuneiform bone, which sup- ports the great toe. The arteries being tied, Mr. Hey applies the flap, which had formed the sole of the foot, to theinteguments which remain at the upper part,find keeps them in contact with sutures. The cicatrix be- ing situated at the top of the foot, is in no danger of being hurt, while the place where the toes were situ-, ated is covered with such strong skin. viz. what pre- viously formed the sole of the foot, that it cannot be injured by any moderate violence—,See Practical Ob- servations in Surgery, p. 535, Sec.) When the metatarsal bone of the great toe is alone diseased, Mr. Hey recommends dissecting it out from the cuneiform bone,'instead of sawing it. The.latter plan cannot be easily accomplished, without removing part of the integuments and muscles, and making a transverse as well as a longitudinal incision These disagreeable things may oe avoided by following the method of Mr. Hey, or that of]Mr.€.Bjft - moving the metatarsal bone, either of the little or great toe, the latter gentleman directs us to ^urry a scalpel round the root of the toe, and then along the side ol the foot. The flaps are then to be dissected back, the metatarsal bone is to be separated from the next, and its square head is to be detached from the tarsus.— (Operative Surgery, .vol. 1, J). 3i)0.) The removal of the central metatarsal and metacar- pal bones is an operation fit much dilliculty, and the sawing of'them is hardly practicable, without injuring tire soit parts. Hence, I am decidedly of opinion with Mr. C. Bell, that instead of a, formal amputation, it is better to extract the diseased botes from the foot or hand, as, indeed, Mr. Hey was in the habit or doing. - That skilful surgeon, I.angenbeck, hoNvever, has da* vised a ready mode of taking away the middle linger with its metacarpal bone from the os magnum, or the. ring-finger,' with its metacarpal bone, from the articu- lation of the latter with the os magnum and os cunei- fonne. In order to find out these articulations, he draws a line from the upper head of the metacarpal bone of the thumb straight across to the metacarpal bone of the finger to be extirpated, and at this place he begins his first incision, winch runs towards each side of the finger like an inverted V. The bone is then separated all round from the soft parts, and dislocated from the carpus, when nothing remains to be done but to cut the parts towards the palm, where the wound is ■also made to resemble an inverted V, but does not ex- tend any farther than is necessary, to complete the se- paration.—\See Langenbeck's Bibl. b. 1, p. 575, and plate 3, f. 1.) This is unquestionably a simple and excellent method of operating, which Langenbeck also recommends as the best way of removing such bones of the metatarsus, as are not situated at the sides of the foot: care being taken tojsave a flap from the sole. It is often difficult, however, to know with certainty whether the disease is confined to the metacarpal or metatarsal bones ; and if it be not, and the carpus or tarsus be affected, the operation will not answer, and amputation be indispensable. This happened in one ' of Langenbeck's cases,'in which he had removed one of the metacarpal bones,,. Modern surgeons never amputate the whole of tho foot or hand, when there is a reasonable chance of preserving any useful portion of it, though the rest may be most severely shattered. Tivus, when a sol- dier had been, struck by a grape-shot, wiiich shattered the metacarpal bones of the little and ring-fingers, grazed the middle finger, and tore up the integuments on the palm and back of the hand, Mr. Guthrie suc- ceeded in saving the twp fingers arid thumb, although, in the removal of the other parts, no regular flaps- could be made for covering the wound.—(On Gun-shot Wounds, p. 382.) In winter campaigns, the toes, and more or less of the foot, are often attacked with morti- fication from cold. In this circumstance, when, the disorder does not extend beyond the middle of the foot or the toes, it is only necessary to cut away the gan- grenous part. On the first entrance of the French army into Holland, alter the revolution, Paroisse met with many of these eases, in which it was'necessary merely to take away the metatarsal bones, or .some- times those of the tars,us< AH the patients operated upon -in this manner for the efi'epts of cold were fcured ; walking afterward with more or less diffi- culty, according as the portion of the foot takemaway • had -been greater or smaller.—(Opuscules de Chir. p. 2180 ■• ' ' , • M. Roux, in his late publication!,tfnds fault with our ignorance of (Jhopart's method of removing.a part of ' the foqt. He-says, Tarn certain, the principal sur- geons in England have never practised, and are -even* totally unacquainted with, the amputation of the foot* at the junction of the two halves of the tarsus, or jhopart's operation.—(Voyage fait, a Loridresen 1814, ou Parallel oe la Chirurgie An'gloise a'vec la C'hirur- gie Franchise, p. 33-,) As it is an operation of consi- derable merit. I think it will be useful to introduce a description of it in the present work. It,is performed in the nearly parallel articulations of the as calcis wilh the os cuboides,, arid of the astragalus with the os na- vicular. Thus the heel is preserved, on which the patient can afterward walk,. The performs e of fc is simple. The tcumiauct iiaviug been appued, the -](https://iiif.wellcomecollection.org/image/b2103719x_0099.jp2/full/800%2C/0/default.jpg)