Surgical treatment of perforation of the bowel in typhoid fever : with a table of 158 cases / W.W. Keen.
- William Williams Keen
- Date:
- [1900]
Licence: In copyright
Credit: Surgical treatment of perforation of the bowel in typhoid fever : with a table of 158 cases / W.W. Keen. Source: Wellcome Collection.
Provider: This material has been provided by The Royal College of Surgeons of England. The original may be consulted at The Royal College of Surgeons of England.
4/16
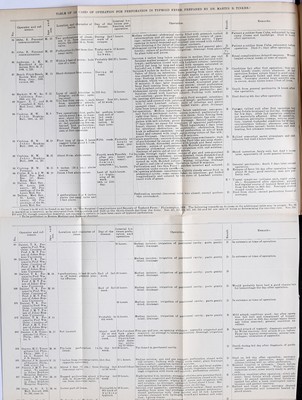
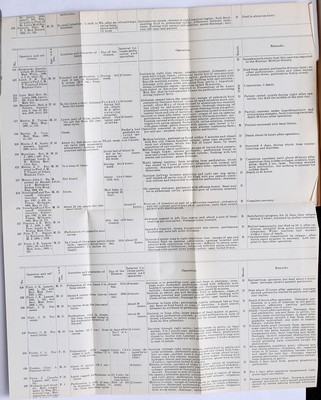
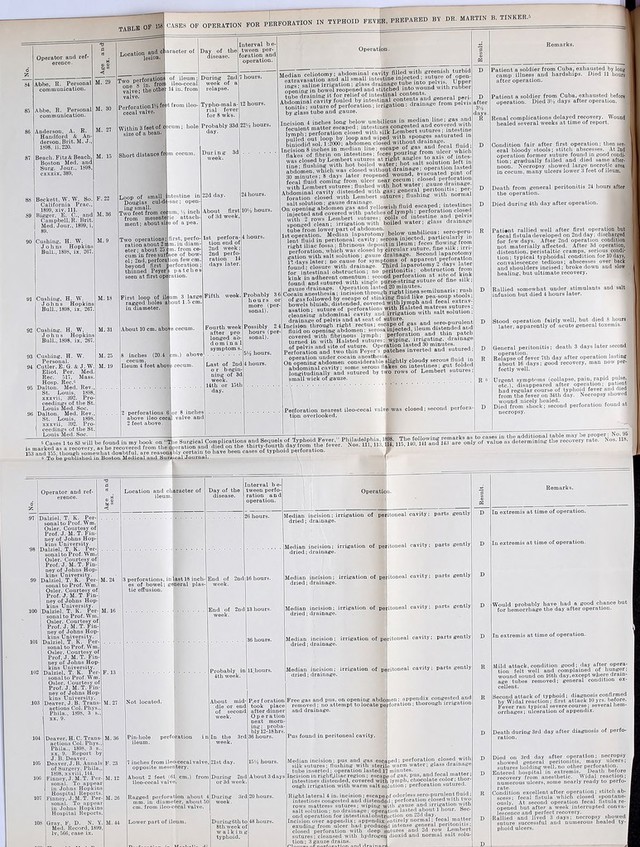
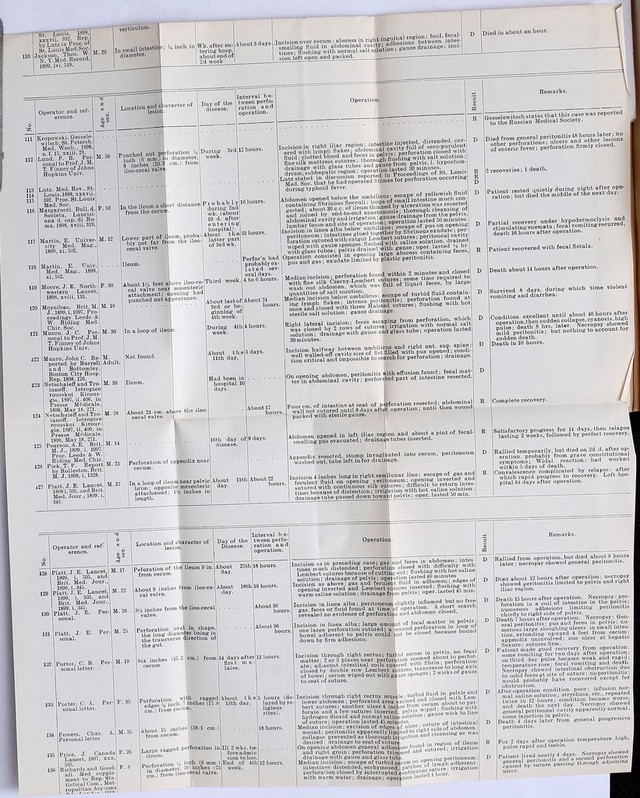
![SnquOp£e,M.E. Bull, et mem. de la Soc. Anat., Paris, 1899, lxxiv, 443. Senn, N. Personal letter. 140 141 142 143 144 jju., uuuuuu, iu.'u Ryan, C. Australa- sian Med.Gaz. 1899. xviii, 334. Senn, N. Personal letter. Taylor, H. M. Va, Med. Semi-Month- ly, iii, 1898-99, 719. Taylor, H. M. Va. Med. Semi-Month- ly. iii, 1898-99, 719, Taylor, H.M. Mary- land Med. Jour.. 1899, xlii, 101. 18 inches from size of a pe«i face of bowel. um; about [j >n free sur- Young adult. In ileum 74 cm. cecal valve; 3 m eter. About 12 inches: circular, puncl ing. ileu Lower part of 12 in. (30.5 cm cecal valve; 2 e on free margi about 4 in. (10 2 m, about from ileo- rforations of bowel cm.) apart. 1 Wanacb, by Willard, De Forest. Annals of Surg,, 1899, xxix, 503, 157 158 15, 1899. Taylor, W J. M. T. Finney. Thurston, E. Haw kins a med. Woch., 189l xxiii, n. f. 15, 21. v. Winiwarter. Rep. A. Polis, Ann, Soc. MCd. Chir. de LiOge, 1897, xxxvi, Wladisslew, C. W. Rep. by Gessele witsch, St. Petersb. med. Woch. 1898, xxiii, n. f. 15, 21. Woodward, S. B. Boston Med. and Surg. Jour., cxxxix, 544. Champlin, S. H. Per- sonal com. The Plexus,” v. 5,164. Champlin,S. H. Per- sonal com. “The Plexus,” v, 5, 164, Champlin, S. H. Per- sonal com. The Plexus” v. 5,164. Saleeby, N. M. Phil- adelphia Medical Jour., 1899, iv, 270. above ileo- m. in diam During 3rd week. 'ove cecum, d-outopen- During 3d week, Aboutthe8th day. 3 days after fever from relapse of 10 days af- ter fever of 6 weeks, Had been sick 6 wlcs. About 14 hours. 4 daya. 15 hours. Several days. About 4 hours. On opening abdominal cavity escape of gas; small intestine dis- tended and congested; covered with flakes of adherent lymph; offensive, turbid fluid with fecal odor in pelvis; ulcer closed by double row Lembert sutures; intestines washed and abdominal cavity und pelvis flushed with hot sterile water; abdomen closed without drainage, Incision in the right flank ; on opening abdomen purulent, odor- less fluid escaped; perforation readily found and sutured; irri- icoa IIUIU , 1.U 1 1 V., 1 <1 gation with boiled water. Celiotomy; perforation and large iutraperitoneal abscess found perforation sutured. Operated for typhoid perforation in two cases. Incision over cecal region; sero-purulent fluid escaped on opening peritoneum; perforation readily found and closed with deep mattress and Lembert sutures; intestines wiped and thorough irrigation with hot saline solution; multiple gauze drainage operation lasted 37 minutes. Median incision; escape of bile-colored serum on opening peri- toneum; perforation closed by deep and superficial sutures; wiping and prolonged irrigation of intestines; gauze drainage; operation lasted about 50 minutes. During anesthesia vomited matter entered th< air passages; death resulted from broncha pneumonia 36 hours after operation. Necropsy showed extensive areas of collapse in lungs; perforation firmly closed; no peritonitis. Death a few minutes after operation; necropsy confirmed diagnosis of typhoid; intestine deeply ulcerated but no other perforations. Recovered from operation and did well fifth day: hemorrhage from another ulcer caused death. One recovery and one death. Convalescence uneventful. Lived but a few hours after operation. Death about 9 hours after operation; thought to be due to acute suppression of urine. Pa- tient had specific urethritis when taken with fever. Age and sex. Location and ch lesion aracter of - M. 34 About 10 in. frorr ileo-cecal e valve. Size lea pencil. - M. 47 About 8 inches fr pin-head openit g. . M. 26 Perforation 5 mn ter, edges sharp 8 in. (20.4 cm.) . in diame- ly marked; above ileo- F. 11 Perforation in an wall; >0 inch in surrounded by tissue. erior cecal diameter, indurated M. 43 8 inches from cy and outline of a cum; size mall bean. M. 24 Two perforations, 21.6 cm. and 41.6 cm. from cecum. M. 1 in (10.2 cm.) above ileo-ce- cal valve; just large enough to admit grooved director. M. 18 1 perforations found in small intestine near cecum. M. 18 Small intestine; opposite mesentery; size of a pea. M. 10 Perforation not found. M. 22 Perforation of ileum, about 30 cm. from ileo-cecal valve. M. Perforation 20 cm. cecal valve. from ileo- M. Pin-hole perforation in thick- ] ened and inflamed Peyer’s patch, 18 in. from ileo-cecal valve. Day of the About day. 24th day. 41st day. About 15 hours, 19 days after confined to bed; ill several days before. About end of 2d week. 15th day. Interval be- tween perfo- ration and operation About 4 hours. Operation. Celiotomy; ulcer invaglnated and 2 rows fine silk sutures inserted . abdominal cavity washed with sterile salt solution; operation lasted 20 minutes. Celiotomy; on opening peritoneal cavity gas and serous fluid escaped; marked general peritonitis; ulcer invaginated and 2 rows silk sutures inserted: abdomen flushed with normal salt solution; drainage introduced and wound closed. Abdomen contained fluid but no feces seen; general peritonitis; perforation sutured; intestines and abdominal cavity wiped abdominal wound left open, packed with gauze. Be tween 5 and 6 hours. ibout the end of 2d week. 14th day. Median, 4-inch incision below umbilicus; on opening peritoneum escape of large amount of sero-purulent fluid with faint fecal' odor; margin of perforation excised; closed by Lembert sutures ; thorough irrigation of abdominal cavity with sterilized water; mopping with marine sponges especially pelvis and lumbar regions; drainage tubes from pelvis and right loin; gauze drain passed upward: operation lasted 25 minutes. Death before abdominal wall was sutured. Patient was in very low condition at time of operation. Death in 24 hours from septic peritonitis. D Condition very bad after operation; rallied somewhat, but died 12 hours later. Median incision; on opening peritoneum escape of gas and thin yellow feces; lymph on intestines “<-1 mocontor,. perforation; closure of perforat on with 2 rows of sutures; abdomen cleansed and closed without drainage. Median incision from umbilicus tj> symphysis; escape of sero- purulent fluid on opening abdomen; peritoneum injected; fibrinous deposits on intestine; perforations closed with Czerny- Lembert suture; numerous antis aptic tampons inserted in all directions; wound left open. ; es :i About 9 Yi hours. Incision in right semilunar line; yellow serum and feces; ileum _ ulcerated areas; perforation clc^si and second continuous sutures; water; large glass drainage tube Median incision; escape of sero-pu: flakes adherent and appearance < tions sutured; operation hastily abdominal cavity because of patien ape of ill smelling, greenish- g:eatly congested, several thin sed by interrupted Lembert , irrigation with hot sterile inserted. irulent fluid with feces; lymph septic peritonitis; perfora- completed by tamponing ;’s baa condition. Perforation not found at operation few days later. Median 3-inch incision; 6 inches , coated with lymph; whitish flupi cavity; edges of perforation excis< Lembert sutures; flushing with without drainage. 1 month. 13th day. About 24 hours. line, Incision; turbid fecal fluid; cavity toneal adhesions, left of median ' tube and gauze drainage. Median incision ; fecal fluid in abdoi. omentum much inflamed; perforate tinuous suture and omental graft peritoneum and drainage. and mesentery in vicinity of but fecal fistula developed a Day after operation condition good; escape of considerable purulent fluid for several days. On fifth day after operation, right parotid bubo developed and abscess of buttock at site of injection of saline solution; 21st day, double otitis media; 24th day, effusion into left knee; 60th day, relapse lasting 14 days; Widal test positive; spleen enlarged. A year after ill- ness patient fat and well. Death 55 hours after operation from peritonitis. Death 18 hours after operation; necropsy con- firmed diagnosis of typhoid fever. of intestine thickened, red, :d and feces in abdominal and closed with double row formal salt solution; suture entered, formed by firm peri , below McBurney’s point minal cavity; intestines and ion closed by transverse con stitched over; toilet of the Operative treatment as in preceding case. Inc.s.on 3?i in. along outer border oF rectus abdominis below um bilicus; escape of straw-colored Serous fluid; longitudinal in- fold of intestinal wall and continuous silk suture, reinforced by continuous catgut suture; 2 other thinned areas sutured; intes- tines wiped; gauze drainage frorn both iliac fossro and from Douglas pouch; operation lasted 1 hour. Patient in very low condition after operation; stimulants and infusion of salt solution un- availing. Death 43 hours after operation; dis- ease of very severe type; at necropsy very numerous intestinal ulcers, abscesses of spleen and mesenteric glands, ulcer of larynx, etc., were found. Death almost immediately after operation. Recovery. Patient nearly moribund at operation; free singulation, oxygen inhalation, elevated foot of bed, etc.-; lived 9 days in typhoid state; no symptoms of peritonitis: wound gangrenous at time of death; abdominal cavity unin- I flamed except slightly in region of sutures. / Recovery; bacteriologic examination demon- j strated. typhoid bacilli, colon bacilli and vari- ous monococci. Widal reaction positive. i Reacted well, but was taken with vomiting and I persistent cough, and died 3 days after opera-1 tion. Necropsy showed suture unchanged ;■ peritonitis limited to pelvis about perfora-B tion; hypostatic congestion of lungs; puru-fl lent infiltration right side chest and abdo-f men; Peyer’s patches all thickened; Widal re-J action positive Bacteriologic examination showed muscles infiltrated with streptococci? In spite of free stimulation patient did not r act and died 10 hours after operation. Slight nausea and vomiting during first dafl after operation, but no pain nor tenderness? nutrient enemata and free stimulation; nl covery from operation was uneventful. Fevif lasted 25 days and relapse 16 days, but eveJ tually perfect recovery,](https://iiif.wellcomecollection.org/image/b22361820_0006.jp2/full/800%2C/0/default.jpg)